Zynteglo: Package Insert / Prescribing Info
Package insert / product label
Generic name: betibeglogene autotemcel
Dosage form: intravenous suspension
Drug class: Miscellaneous uncategorized agents
J Code (medical billing code): J3393 (Per treatment, injection)
Medically reviewed by Drugs.com. Last updated on Dec 13, 2023.
On This Page
- Indications and Usage
- Dosage and Administration
- Dosage Forms and Strengths
- Contraindications
- Warnings and Precautions
- Adverse Reactions/Side Effects
- Drug Interactions
- Use In Specific Populations
- Description
- Clinical Pharmacology
- Nonclinical Toxicology
- Clinical Studies
- References
- How Supplied/Storage and Handling
- Storage and Handling
- Patient Counseling Information
Highlights of Prescribing Information
ZYNTEGLO (betibeglogene autotemcel) suspension for intravenous infusion
Initial U.S. Approval: 2022
Indications and Usage for Zynteglo
ZYNTEGLO is an autologous hematopoietic stem cell-based gene therapy indicated for the treatment of adult and pediatric patients with β-thalassemia who require regular red blood cell (RBC) transfusions. (1)
Zynteglo Dosage and Administration
For autologous use only. For intravenous use only.
- Patients are required to undergo hematopoietic stem cell (HSC) mobilization followed by apheresis to obtain CD34+ cells for ZYNTEGLO manufacturing. (2.2)
- Dosing of ZYNTEGLO is based on the number of CD34+ cells in the infusion bag(s) per kg of body weight. (2.1)
- The minimum recommended dose is 5.0 × 106 CD34+ cells/kg. (2.1)
- Full myeloablative conditioning must be administered before infusion of ZYNTEGLO. (2.2)
- Prophylaxis for hepatic veno-occlusive disease (VOD) is recommended. Prophylaxis for seizures should be considered. (2.2)
- Verify that the patient's identity matches the unique patient identification information on the ZYNTEGLO infusion bag(s) prior to infusion. (2.2)
- Do not sample, alter, or irradiate ZYNTEGLO. (2.2)
- Do not use an in-line blood filter or an infusion pump. (2.3)
- Administer each infusion bag of ZYNTEGLO via intravenous infusion over a period of less than 30 minutes. (2.3)
Dosage Forms and Strengths
Contraindications
None. (4)
Warnings and Precautions
- Delayed Platelet Engraftment: Monitor platelet counts until platelet engraftment and recovery are achieved. Patients should be monitored for thrombocytopenia and bleeding. (5.1)
- Risk of Neutrophil Engraftment Failure: Monitor absolute neutrophil counts (ANC) after ZYNTEGLO infusion. If neutrophil engraftment does not occur administer rescue cells. (5.2)
- Risk of Insertional Oncogenesis: Monitor patients at least annually for hematologic malignancies for at least 15 years after ZYNTEGLO infusion. (5.3)
- Hypersensitivity Reactions: Monitor for hypersensitivity reactions during infusion. (5.4)
Adverse Reactions/Side Effects
The most common non-laboratory adverse reactions (incidence ≥ 20%) were mucositis, febrile neutropenia, vomiting, pyrexia (fever), alopecia (hair loss), epistaxis (nose bleed), abdominal pain, musculoskeletal pain, cough, headache, diarrhea, rash, constipation, nausea, decreased appetite, pigmentation disorder, and pruritus (itch). (6.1)
The most common Grade 3 or 4 laboratory abnormalities (> 50%) include neutropenia, thrombocytopenia, leukopenia, anemia, and lymphopenia. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact bluebird bio at 1-833-999-6378 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
- Anti-retrovirals and Hydroxyurea: Do not take anti-retroviral medications or hydroxyurea for one month prior to mobilization, or for the expected duration for elimination of the medications, and until all cycles of apheresis are completed (7.2)
- Iron Chelation: Discontinue iron chelators 7 days prior to initiation of myeloablative conditioning. Avoid use of myelosuppressive iron chelators for 6 months after ZYNTEGLO infusion. (7.3)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 8/2022
Full Prescribing Information
1. Indications and Usage for Zynteglo
ZYNTEGLO is indicated for the treatment of adult and pediatric patients with β-thalassemia who require regular red blood cell (RBC) transfusions.
2. Zynteglo Dosage and Administration
For autologous use only. For one-time single-dose intravenous use only.
2.1 Dose
ZYNTEGLO is provided as a single dose for infusion containing a suspension of CD34+ cells in one or more infusion bags. The minimum recommended dose of ZYNTEGLO is 5.0 × 106 CD34+ cells/kg.
See the Lot Information Sheet provided with the product shipment for additional information pertaining to dose.
2.2 Preparation Before ZYNTEGLO Infusion
Before mobilization, apheresis, and myeloablative conditioning are initiated, confirm that hematopoietic stem cell (HSC) transplantation is appropriate for the patient.
It is recommended that patients be maintained at a hemoglobin (Hb) ≥ 11 g/dL for at least 30 days prior to mobilization and 30 days prior to myeloablative conditioning.
Granulocyte-colony stimulating factor (G-CSF) and plerixafor were used for mobilization and busulfan was used for myeloablative conditioning. Refer to the prescribing information for the mobilization agent(s) and the myeloablative conditioning agent(s) prior to treatment.
Perform screening for hepatitis B virus (HBV), hepatitis C virus (HCV), human T-lymphotrophic virus 1 & 2 (HTLV-1/HTLV-2), and human immunodeficiency virus 1 & 2 (HIV-1/HIV-2) in accordance with clinical guidelines before collection of cells for manufacturing.
Mobilization and Apheresis
Patients are required to undergo HSC mobilization followed by apheresis to obtain CD34+ cells for product manufacturing.
The target number of CD34+ cells to be collected is ≥ 12 × 106 CD34+ cells/kg. If the minimum dose of 5.0 × 106 CD34+ cells/kg is not met, the patient may undergo additional cycles of mobilization and apheresis, separated by at least 14 days, in order to obtain more cells for additional manufacture. Up to two drug product lots may be administered to meet the target dose.
A back-up collection of CD34+ cells of ≥ 1.5 × 106 CD34+ cells/kg (if collected by apheresis) or > 1.0 × 108 TNC/kg (Total Nucleated Cells, if collected by bone marrow harvest) is required. These cells must be collected from the patient and be cryopreserved prior to myeloablative conditioning. The back-up collection may be needed for rescue treatment if there is: 1) compromise of hematopoietic stem cells or ZYNTEGLO before infusion, 2) primary engraftment failure, or 3) loss of engraftment after infusion with ZYNTEGLO.
Myeloablative Conditioning
Full myeloablative conditioning must be administered before infusion of ZYNTEGLO. Consult prescribing information for the myeloablative conditioning agent(s) prior to treatment.
Stop iron chelation at least 7 days prior to myeloablative conditioning. Prophylaxis for hepatic veno-occlusive disease (VOD) is recommended [see Clinical Studies (14)]. Prophylaxis for seizures should be considered, as appropriate.
Do not begin myeloablative conditioning until the complete set of infusion bag(s) constituting the dose of ZYNTEGLO has been received and stored at the treatment center and the availability of the back-up collection is confirmed. After completion of the myeloablative conditioning, allow a minimum of 48 hours of washout before ZYNTEGLO infusion.
Receipt and Storage of ZYNTEGLO
- ZYNTEGLO is shipped to the treatment center in the vapor phase of liquid nitrogen shipper.
- Confirm patient identifiers on the product label(s) and Lot Information Sheet within the shipper.
- If there are any concerns about the product or packaging upon receipt, contact bluebird bio at 1-833-999-6378.
- Keep the infusion bag(s) in the metal cassette(s) and transfer ZYNTEGLO from the vapor phase of liquid nitrogen shipper to the treatment center vapor phase of liquid nitrogen storage at ≤ -140°C (≤ -220°F). Store in the vapor phase of liquid nitrogen at ≤ -140°C (≤ -220°F) until ready for thaw and administration.
Preparation of ZYNTEGLO for Infusion
Coordinate the timing of ZYNTEGLO thaw and infusion. Confirm the infusion time in advance and adjust the start time of ZYNTEGLO thaw such that it will be available for infusion when the patient and healthcare providers are ready.
- 1.
- Remove each metal cassette from liquid nitrogen storage and remove each infusion bag from the metal cassette.
- 2.
- Confirm that ZYNTEGLO is printed on the infusion bag(s).
- 3.
- Confirm that patient identity matches the unique patient identifiers located on the ZYNTEGLO infusion bag(s). Do not infuse ZYNTEGLO if the information on the patient-specific label on the infusion bag does not match the intended patient, and contact bluebird bio at 1-833-999-6378.
- 4.
- Ensure the correct number of infusion bags are present. Use the accompanying Lot Information Sheet to confirm that each infusion bag is within the expiration date.
- 5.
- Inspect each infusion bag for any breaches of integrity before thawing and infusion. If an infusion bag is compromised, follow the local guidelines and contact bluebird bio immediately at 1-833-999-6378.
- 6.
- If more than one infusion bag is provided, thaw and administer each infusion bag completely before proceeding to thaw the next infusion bag.
- 7.
- Thaw ZYNTEGLO at 37°C (98.6°F) in a water bath or dry bath. Thawing of each infusion bag takes approximately 2 to 4 minutes. Do not leave ZYNTEGLO unattended. Do not submerge the infusion ports in a water bath.
- 8.
- After thaw, mix the contents gently by massaging the infusion bag to disperse clumps of cellular material until all of the contents are uniform. If visible cell clumps remain, continue to gently mix the contents of the bag. Most small clumps of cellular material should disperse with gentle manual mixing. Do not filter, wash, spin down and/or resuspend ZYNTEGLO in new media prior to infusion.
- 9.
- Do not sample, alter, irradiate or refreeze ZYNTEGLO.
2.3 Administration
ZYNTEGLO is for autologous use only. The patient's identity must match the patient identifiers on the ZYNTEGLO cassette(s) and infusion bag(s). Do not infuse ZYNTEGLO if the information on the patient-specific label does not match the intended patient.
- Product must be administered within 4 hours after thawing.
- Do not use an in-line blood filter or an infusion pump.
- 1.
- Before infusion, confirm that the patient's identity matches the unique patient identifiers on the ZYNTEGLO infusion bag(s). Use the Lot Information Sheet to confirm the total number of infusion bags to be administered.
- 2.
- Expose the sterile port on the infusion bag by tearing off the protective wrap covering the port.
- 3.
- Access the infusion bag and infuse ZYNTEGLO as soon as possible after thawing and complete the infusion within 4 hours.
- 4.
- Administer each infusion bag of ZYNTEGLO via intravenous infusion over a period of less than 30 minutes. If more than one infusion bag is provided, administer each infusion bag completely before proceeding to thaw and infuse the next infusion bag.
- 5.
- Flush all ZYNTEGLO remaining in the infusion bag(s) and any associated tubing with at least 50 mL of 0.9% sodium chloride solution to ensure that as many cells as possible are infused into the patient.
After ZYNTEGLO Administration
Standard procedures for patient management after HSC transplantation should be followed after ZYNTEGLO infusion.
- Irradiate any blood products required within the first 3 months after ZYNTEGLO infusion.
- Granulocyte-colony stimulating factor (G-CSF) is not recommended for 21 days after ZYNTEGLO infusion.
- Restarting iron chelation after ZYNTEGLO infusion may be necessary and should be based on clinical practice [see Drug Interactions (7.3) and Clinical Studies (14)]. Phlebotomy can be used in lieu of iron chelation, when appropriate.
- Patients should not donate blood, organs, tissues, or cells at any time in the future.
ZYNTEGLO contains human blood cells that are genetically modified with replication-incompetent, self-inactivating lentiviral vector. Follow universal precautions and biosafety guidelines (Biosafety Level 2) for handling and disposal of ZYNTEGLO to avoid potential transmission of infectious diseases.
3. Dosage Forms and Strengths
ZYNTEGLO is a cell suspension for intravenous infusion.
ZYNTEGLO is composed of up to four infusion bags which contain 2.0 to 20 × 106 cells/mL suspended in cryopreservation solution [see How Supplied/Storage and Handling (16)]. Each infusion bag contains approximately 20 mL of ZYNTEGLO. A single dose of ZYNTEGLO contains a minimum of 5.0 × 106 CD34+ cells per kg of body weight, suspended in cryopreservation solution.
See the Lot Information Sheet for actual dose.
5. Warnings and Precautions
5.1 Delayed Platelet Engraftment
Delayed platelet engraftment has been observed with ZYNTEGLO treatment. Bleeding risk is increased prior to platelet engraftment and may continue after engraftment in patients with prolonged thrombocytopenia; 15% of patients had ≥ Grade 3 decreased platelets on or after Day 100.
Patients should be made aware of the risk of bleeding until platelet recovery has been achieved. Monitor patients for thrombocytopenia and bleeding according to standard guidelines. Conduct frequent platelet counts until platelet engraftment and platelet recovery are achieved. Perform blood cell count determination and other appropriate testing whenever clinical symptoms suggestive of bleeding arise.
5.2 Risk of Neutrophil Engraftment Failure
There is a potential risk of neutrophil engraftment failure after treatment with ZYNTEGLO. Neutrophil engraftment failure is defined as failure to achieve three consecutive absolute neutrophil counts (ANC) ≥ 500 cells/microliter obtained on different days by Day 43 after infusion of ZYNTEGLO. Monitor neutrophil counts until engraftment has been achieved. If neutrophil engraftment failure occurs in a patient treated with ZYNTEGLO, provide rescue treatment with the back-up collection of CD34+ cells.
5.3 Risk of Insertional Oncogenesis
There is a potential risk of lentiviral vector (LVV)-mediated insertional oncogenesis after treatment with ZYNTEGLO.
Patients treated with ZYNTEGLO may develop hematologic malignancies and should be monitored lifelong. Monitor for hematologic malignancies with a complete blood count (with differential) at Month 6 and Month 12 and then at least annually for at least 15 years after treatment with ZYNTEGLO, and integration site analysis at Months 6, 12, and as warranted.
In the event that a malignancy occurs, contact bluebird bio at 1-833-999-6378 for reporting and to obtain instructions on collection of samples for testing.
5.4 Hypersensitivity Reactions
Allergic reactions may occur with the infusion of ZYNTEGLO. The dimethyl sulfoxide (DMSO) in ZYNTEGLO may cause hypersensitivity reactions, including anaphylaxis.
5.5 Anti-retroviral and Hydroxyurea Use
Patients should not take prophylactic HIV anti-retroviral medications or hydroxyurea for at least one month prior to mobilization, or for the expected duration for elimination of the medications, and until all cycles of apheresis are completed [see Drug Interactions (7.2)].
If a patient requires anti-retrovirals for HIV prophylaxis, then confirm a negative test for HIV before beginning mobilization and apheresis of CD34+ cells.
5.6 Interference with Serology Testing
Patients who have received ZYNTEGLO are likely to test positive by polymerase chain reaction (PCR) assays for HIV due to integrated BB305 LVV proviral DNA, resulting in a false-positive test for HIV. Therefore, patients who have received ZYNTEGLO should not be screened for HIV infection using a PCR-based assay.
6. Adverse Reactions/Side Effects
The following adverse reactions are described elsewhere in the labeling:
- Delayed Platelet Engraftment [see Warnings and Precautions (5.1)]
- Risk of Neutrophil Engraftment Failure [see Warnings and Precautions (5.2)]
- Risk of Insertional Oncogenesis [see Warnings and Precautions (5.3)]
- Hypersensitivity Reactions [see Warnings and Precautions (5.4)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety data described in this section reflect exposure to ZYNTEGLO in two open-label, single-arm clinical trials and one long-term follow-up study, in which 41 patients with β-thalassemia requiring regular transfusions were treated with ZYNTEGLO [see Clinical Studies (14)]. The median (min, max) age across the trials was 13 (4, 34) years; 49% were females; 49% were Asian, 44% White, 5% Other, 2% Not Reported. The median (min, max) duration of follow-up was 27.2 (4.1, 48.2) months.
In the two trials, serious adverse reactions occurred in 37% of patients as of last follow-up. The most common serious adverse reactions (> 3%) were pyrexia (fever), thrombocytopenia, liver veno-occlusive disease, febrile neutropenia, neutropenia, and stomatitis. There were no deaths.
The most common adverse reactions (≥ 20%) were mucositis, febrile neutropenia, vomiting, pyrexia (fever), alopecia (hair loss), epistaxis (nose bleed), abdominal pain, musculoskeletal pain, cough, headache, diarrhea, rash, constipation, nausea, decreased appetite, pigmentation disorder, and pruritus (itch).
Table 1 presents the non-laboratory treatment emergent adverse reactions reported in at least 10% of patients and Table 2 describes the laboratory abnormalities of Grade 3 or 4 that occurred in at least 10% of patients.
| Adverse Reaction | % Any Grade | % Grade 3 or Higher |
|---|---|---|
|
||
| Blood and lymphatic system disorders | ||
| Febrile neutropenia | 51 | 51 |
| Gastrointestinal disorders | ||
| Mucositis†‡ | 95 | 63 |
| Vomiting | 49 | 0 |
| Abdominal pain§ | 39 | 2 |
| Diarrhea | 27 | 0 |
| Nausea | 24 | 2 |
| Constipation | 24 | 0 |
| Dyspepsia | 10 | 5 |
| Gingival bleeding | 10 | 2 |
| General disorders and administration site conditions | ||
| Pyrexia | 49 | 12 |
| Fatigue | 12 | 0 |
| Hepatobiliary disorders | ||
| Venoocclusive liver disease | 10 | 7 |
| Infections and infestations | ||
| Viral infection¶ | 17 | 2 |
| Upper respiratory tract infections#‡ | 15 | 0 |
| Nasopharyngitis | 12 | 0 |
| SepsisÞ | 10 | 10 |
| Injury, poisoning and procedural complications | ||
| Procedural pain | 15 | 0 |
| Transfusion reaction | 15 | 0 |
| Metabolism and nutrition disorders | ||
| Decreased appetite | 24 | 15 |
| Musculoskeletal and connective tissue disorders | ||
| Musculoskeletal pain߇ | 37 | 0 |
| Nervous system disorders | ||
| Headacheà | 29 | 0 |
| Respiratory, thoracic and mediastinal disorders | ||
| Epistaxis | 42 | 20 |
| Coughè | 34 | 0 |
| Oropharyngeal painð‡ | 15 | 0 |
| Dyspnea | 12 | 0 |
| Hypoxia | 12 | 7 |
| Rhinitisø | 12 | 0 |
| Skin and subcutaneous tissue disorders | ||
| Alopecia | 44 | 0 |
| Rashý‡ | 27 | 0 |
| Pigmentation disorder£ | 24 | 0 |
| Pruritus | 22 | 0 |
| Vascular disorders | ||
| Hypertension | 10 | 0 |
Other clinically important adverse reactions that occurred in less than 10% of patients include the following:
Cardiac disorders: congestive heart failure (2%)
Hepatobiliary disorders: Serious hepatic veno-occlusive disease (VOD) occurred in 3 (7%) patients; of these three, two had not received prophylaxis for VOD. All patients who experienced serious VOD received treatment with defibrotide and recovered. Patients with β-thalassemia requiring regular transfusions may be at an increased risk of VOD following myeloablative conditioning.1
Infections and infestations: pneumonia (7%)
Infusion-related reaction including abdominal pain (7%) and tachycardia (2%).
| Laboratory Abnormality‡ | Grade 3 or 4 (%) |
|---|---|
| Abbreviations: ALT: alanine aminotransferase | |
| Neutropenia | 100 |
| Thrombocytopenia | 100 |
| Leukopenia | 100 |
| Anemia | 95 |
| Lymphopenia | 61 |
| ALT Increased | 24 |
| Hypophosphatemia | 20 |
| Hyperglycemia | 14 |
| Hypokalemia | 12 |
| Hyperbilirubinemia | 10 |
| Hyponatremia | 10 |
Platelet Engraftment Delay
Platelet engraftment was defined as three consecutive platelet values ≥ 20,000 cells/microliter, obtained on different days after ZYNTEGLO infusion, with no platelet transfusions administered for 7 days immediately preceding and during the evaluation period. Forty-one patients treated with ZYNTEGLO achieved platelet engraftment by a median of Day 46 (range 20 - 94) in clinical studies. Patients without a spleen reached the criterion for platelet engraftment earlier as compared to patients with an intact spleen: median Day 42 (range, 21 - 53 days) vs. median Day 50 (range, 20 - 94 days), respectively. Patients achieving platelet engraftment at ≥ Day 46 did not have an increased incidence of bleeding compared with patients with platelet engraftment at < Day 46.
Neutrophil Engraftment
While all subjects achieved neutrophil engraftment after ZYNTEGLO in the clinical studies, 7% of patients remained dependent on G-CSF beyond Day 43, one through Day 77. G-CSF discontinuation was followed by transient decreases in neutrophil counts to < 500 cells/microliter after Day 43 in six (15%) patients.
7. Drug Interactions
No formal drug interaction studies have been performed. ZYNTEGLO is not expected to interact with the hepatic cytochrome P-450 family of enzymes or drug transporters.
7.1 Live Vaccines
Follow institutional guidelines for vaccine administration. The safety of immunization with live viral vaccines during or following ZYNTEGLO treatment has not been studied.
7.2 Anti-retrovirals and Hydroxyurea
Patients should not take anti-retroviral medications or hydroxyurea for at least one month prior to mobilization or the expected duration for elimination of the medications, and until all cycles of apheresis are completed [see Warnings and Precautions (5.5)]. Anti-retroviral medications may interfere with manufacturing of the apheresed cells.
7.3 Iron Chelation
Drug-drug interactions between iron chelators and the myeloablative conditioning agent must be considered. Iron chelators should be discontinued at least 7 days prior to initiation of conditioning. The prescribing information for the iron chelator(s) and the myeloablative conditioning agent should be consulted for the recommendations regarding co-administration with CYP3A substrates.
Some iron chelators are myelosuppressive. After ZYNTEGLO infusion, avoid use of these iron chelators for 6 months. If iron chelation is needed, consider administration of non-myelosuppressive iron chelators. Phlebotomy can be used in lieu of iron chelation, when appropriate [see Clinical Studies (14)].
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
There are no available data with ZYNTEGLO administration in pregnant women. Consider the risks associated with myeloablative conditioning agents on pregnancy and fertility.
No reproductive and developmental toxicity studies in animals have been conducted with ZYNTEGLO to assess whether it can cause fetal harm when administered to a pregnant woman. It is not known whether ZYNTEGLO has the potential to be transferred to the fetus. Therefore, ZYNTEGLO should not be administered to women who are pregnant, and pregnancy after ZYNTEGLO infusion should be discussed with the treating physician.
No nonclinical germline transmission studies have been conducted with ZYNTEGLO.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
8.2 Lactation
Risk Summary
There is no information regarding the presence of ZYNTEGLO in human milk, the effect on the breastfed infant, and the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for ZYNTEGLO and any potential adverse effects on the breastfed child from ZYNTEGLO. Therefore, ZYNTEGLO is not recommended for women who are breastfeeding, and breastfeeding after ZYNTEGLO infusion should be discussed with the treating physician.
8.3 Females and Males of Reproductive Potential
Pregnancy Testing
A negative serum pregnancy test must be confirmed prior to the start of mobilization and re-confirmed prior to conditioning procedures and before ZYNTEGLO administration.
Contraception
There are insufficient exposure data to provide a precise recommendation on duration of contraception following treatment with ZYNTEGLO.
Women of childbearing potential and men capable of fathering a child should use an effective method of contraception (intra-uterine device or combination of hormonal and barrier contraception) from start of mobilization through at least 6 months after administration of ZYNTEGLO. Advise patients of the risks associated with conditioning agents.
8.4 Pediatric Use
The safety and efficacy of ZYNTEGLO have been established in pediatric patients with β-thalassemia requiring regular transfusions. Use of ZYNTEGLO is supported by two Phase 3 studies [see Clinical Studies (14)] that included 27 pediatric patients in the following age groups: 16 children (less than 12 years) and 11 adolescents (age 12 years to less than 18 years).
No differences in efficacy or clinical safety were observed between the adult and pediatric subgroups. Engraftment times were longer in pediatric patients, but not associated with increases in infections or bleeding events. The median (min, max) time to neutrophil engraftment for patients less than 18 years was 26 (16, 39) days versus 21 (13, 27) days for patients 18 years or older. The median (min, max) time to platelet engraftment for patients less than 18 years was 50 (20, 94) days versus 43 (21, 58) days for patients 18 years or older. Longer engraftment time was associated with intact spleens.
The safety and efficacy of ZYNTEGLO in children less than 4 years of age have not been established. No data are available.
8.5 Geriatric Use
ZYNTEGLO has not been studied in patients > 65 years of age. Hematopoietic stem cell (HSC) transplantation must be appropriate for a patient to be treated with ZYNTEGLO.
8.6 Patients Seropositive for Human Immunodeficiency Virus (HIV)
ZYNTEGLO has not been studied in patients with HIV-1, HIV-2, HTLV-1, or HTLV-2. A negative serology test for HIV is necessary to ensure acceptance of apheresis material for ZYNTEGLO manufacturing. Apheresis material from patients with a positive test for HIV will not be accepted for ZYNTEGLO manufacturing.
11. Zynteglo Description
ZYNTEGLO (betibeglogene autotemcel) is a βA-T87Q-globin gene therapy consisting of autologous CD34+ cells, containing hematopoietic stem cells (HSCs), transduced with BB305 LVV encoding βA-T87Q-globin, suspended in cryopreservation solution. ZYNTEGLO is intended for one-time administration to add functional copies of a modified form of the β-globin gene (βA-T87Q-globin gene) into the patient's own HSCs.
ZYNTEGLO is prepared from the patient's own HSCs, which are collected via apheresis procedure(s). The autologous cells are enriched for CD34+ cells, then transduced ex vivo with BB305 LVV, a self-inactivating LVV. The promoter, a regulatory element of the LVV that controls the expression of the transgene selected for BB305 LVV, is a cellular (non-viral) promoter that controls gene expression specific to the erythroid lineage cells (red blood cells and their precursors). BB305 LVV encodes βA-T87Q-globin. The transduced CD34+ cells are washed, formulated into a suspension, and then cryopreserved. ZYNTEGLO is frozen in a patient-specific infusion bag(s) and is thawed prior to administration [see Dosage and Administration (2.2), How Supplied/Storage and Handling (16)]. The thawed product is colorless to white to red, including shades of white or pink, light yellow, and orange, and may contain small proteinaceous particles. Due to the presence of cells, the solution may be clear to slightly cloudy and may contain visible cell aggregates.
The formulation contains 5% dimethyl sulfoxide (DMSO).
12. Zynteglo - Clinical Pharmacology
12.1 Mechanism of Action
ZYNTEGLO adds functional copies of a modified β-globin gene into patients' hematopoietic stem cells (HSCs) through transduction of autologous CD34+ cells with BB305 LVV. After ZYNTEGLO infusion, transduced CD34+ HSCs engraft in the bone marrow and differentiate to produce RBCs containing biologically active βA-T87Q-globin (a modified β-globin protein) that will combine with α-globin to produce functional adult Hb containing βA-T87Q-globin (HbAT87Q). βA-T87Q-globin can be quantified relative to other globin species in peripheral blood using high-performance liquid chromatography. βA-T87Q-globin expression is designed to correct the β/α-globin imbalance in erythroid cells of patients with β-thalassemia and has the potential to increase functional adult HbA and total Hb to normal levels and eliminate dependence on regular pRBC transfusions.
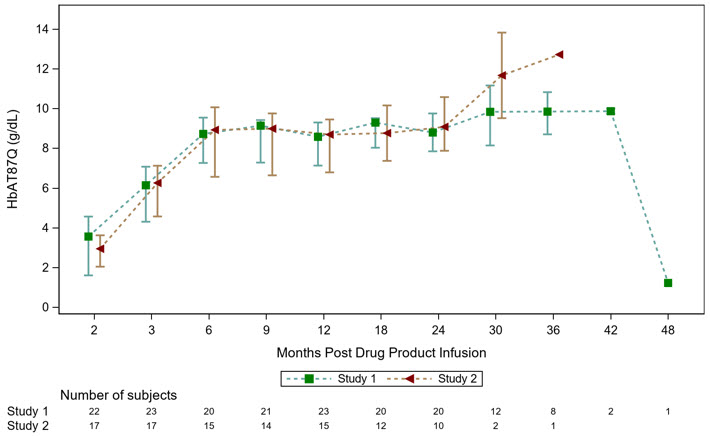
12.2 Pharmacodynamics
HbAT87Q generally increased steadily after ZYNTEGLO infusion and stabilized by approximately Month 6 after infusion (Figure 1). Patients had a Month 6 median (min, max) HbAT87Q of 8.7 (0.0, 12.0) g/dL in the ongoing Phase 3 studies, Study 1 and Study 2 (N = 35).
HbAT87Q remained durable with a median (min, max) of 8.8 (0.3, 12.4) g/dL at Month 24 in the ongoing Phase 3 studies (N = 30). HbAT87Q in the Phase 3 studies continued to remain durable at last follow-up through Month 36, demonstrating sustained expression of the βA-T87Q protein derived from irreversible integration of the βA-T87Q-globin gene into long-term hematopoietic stem cells (HSCs).
12.3 Pharmacokinetics
ZYNTEGLO is an autologous gene therapy which includes hematopoietic stem cells (HSCs) that have been genetically modified ex vivo. The nature of ZYNTEGLO is such that conventional studies on pharmacokinetics, absorption, distribution, metabolism, and elimination are not applicable.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No carcinogenicity studies have been performed with ZYNTEGLO. Intravenous administration of ZYNTEGLO in a mouse model of β-thalassemia showed no evidence of toxicity, genotoxicity, or oncogenesis (tumorigenicity).
No studies have been conducted to evaluate the effects of ZYNTEGLO on fertility.
14. Clinical Studies
The efficacy of ZYNTEGLO was evaluated in 2 ongoing Phase 3 open-label, single-arm, 24-month, multicenter studies (Study 1 and Study 2) in 41 patients aged 4 to 34 years with β-thalassemia requiring regular transfusions. Following completion of the 24-month parent studies, patients were invited to enroll in an ongoing long-term safety and efficacy follow-up study for an additional 13 years (Study 3).
Patients were considered to be eligible for the Phase 3 studies if they had a history of transfusions of at least 100 mL/kg/year of packed red blood cells (pRBCs) or with 8 or more transfusions of pRBCs per year in the 2 years preceding enrollment. Table 3 includes the demographics and characteristics for patients in the Phase 3 studies.
| Study 1 N = 23 | Study 2 N = 18 |
|
|---|---|---|
|
||
| Genotype | non-β0/β0 | β0/β0 or non-β0/β0
(12 β0/β0; 6 non-β0/β0) |
| Age, years
Median (min, max) | 15 (4, 34) | 13 (4, 33) |
| Sex | 52% females; 48% males | 44% females: 56% males |
| Race | ||
| Asian | 57% | 39% |
| White | 35% | 56% |
| Other/Not Reported | 9% | 6% |
| Baseline* transfusion volume, mL/kg/year
Median (min, max) | 208 (142, 274) | 194 (75, 289) |
| Baseline* transfusion frequency, transfusions per year
Median (min, max) | 16 (12, 37) | 17 (11, 40) |
| Lansky or Karnofsky Performance Score
All patients, minimum score Percentage of patients with score of 100 | ≥ 80 52% | ≥ 90 56% |
| Cardiac T2* at baseline, msec
Median (min, max) | 37 (21, 57) | 37 (15, 75) |
| Serum Ferritin at baseline, pmol/L
Median (min, max) | 4438 (784, 22517) | 3275 (1279, 8874) |
| Liver Iron concentration at baseline, mg/g
Median (min, max) | 5.3 (1.0, 41.0) | 3.6 (1.2, 13.2) |
Patients who had severely elevated iron in the heart (i.e., patients with cardiac T2* less than 10 msec by magnetic resonance imaging [MRI]) or advanced liver disease were not accepted into the studies. MRI of the liver was performed on all patients. Patients older than 18 years with MRI results demonstrating liver iron content ≥ 15 mg/g underwent liver biopsy for further evaluation. Patients younger than 18 years with MRI results demonstrating liver iron content ≥ 15 mg/g were excluded from the studies unless a liver biopsy (at the discretion of the investigator) could provide additional data to confirm eligibility. Patients with a liver biopsy demonstrating bridging fibrosis, cirrhosis, or active hepatitis, were also excluded.
Mobilization and Apheresis
All patients were administered G-CSF and plerixafor to mobilize stem cells prior to the apheresis procedure. The planned dose of G-CSF was 10 µg/kg/day in patients with a spleen, and 5 µg/kg/day in patients without a spleen, given in the morning on Days 1 through 5 of mobilization. The planned dose of plerixafor was 0.24 mg/kg/day, given in the evening on Days 4 and 5 of mobilization. Apheresis generally occurred on mobilization Day 5 and 6 and if a third day of collection was needed, plerixafor and G-CSF dosing was extended to Day 6. The dose of G-CSF was decreased by half if the white blood cell (WBC) count exceeded 100 × 109/L prior to the day of apheresis. Most patients collected the minimum number of CD34+ cells to manufacture ZYNTEGLO with 1 cycle of mobilization and apheresis.
Pre-treatment Conditioning
All patients received full myeloablative conditioning with busulfan prior to treatment with ZYNTEGLO. The planned dose of busulfan was 3.2 mg/kg/day for patients 18 years and older as a 3-hour IV infusion daily for 4 consecutive days with a recommended target AUC0-24h of 3800-4500 µM*min. The planned dose of busulfan was 0.8 mg/kg for patients younger than 18 years of age as a 2-hour IV infusion every 6 hours for a total of 16 doses with a recommended target of AUC0-6h of 950-1125 µM*min.
The busulfan prescribing information was used for information on the appropriate method for determination of patient weight-based dosing. Busulfan dose adjustments were made as needed based on pharmacokinetic monitoring. In the clinical studies after completion of the 4-day course of busulfan, a washout period of at least 48 hours was required before ZYNTEGLO administration. Busulfan levels were measured 48 hours after final dose of busulfan for retrospective confirmation of adequate washout.
All patients received anti-seizure prophylaxis with agents other than phenytoin prior to initiating busulfan. Phenytoin was not used for anti-seizure prophylaxis because of its induction of cytochrome P450 and resultant increased clearance of busulfan.
Prophylaxis for hepatic veno-occlusive disease (VOD)/hepatic sinusoidal obstruction syndrome was required with ursodeoxycholic acid or defibrotide, per institutional guidelines.
ZYNTEGLO Administration
All patients (N = 41) were administered ZYNTEGLO with a median (min, max) dose of 9.4 (5.0, 42.1) × 106 CD34+ cells/kg as an intravenous infusion.
After ZYNTEGLO Administration
G-CSF was not recommended for 21 days after ZYNTEGLO infusion in Phase 3 studies. A total of 24% of patients (N = 10/41) received G-CSF within 21 days after ZYNTEGLO infusion.
Neutrophil engraftment was reported on median (min, max) Day 26 (13, 39) after ZYNTEGLO infusion.
As ZYNTEGLO is an autologous therapy, long-term immunosuppressive agents were not required in clinical studies.
Study 1
Study 1 (NCT02906202) is an ongoing Phase 3 open-label, single-arm, 24-month study to evaluate the efficacy of ZYNTEGLO in 23 patients with β-thalassemia requiring regular transfusions and with a non-β0/β0 genotype. Nineteen out of 23 patients have rolled over into a long-term follow-up study (Study 3, NCT02633943) after Month 24.
The median (min, max) duration of follow-up is 29.5 (13.0, 48.2) months. All patients remain alive at last follow-up. There were no cases of graft versus-host disease (GVHD), graft failure, or graft rejection in the clinical studies.
The benefit of ZYNTEGLO was established based on achievement of transfusion independence (TI), defined as a weighted average Hb ≥ 9 g/dL without any pRBC transfusions for a continuous period of ≥ 12 months at any time during the study, after infusion of ZYNTEGLO. Of 22 patients evaluable for TI, 20 (91%, 95% CI: 71, 99) achieved TI with a median (min, max) weighted average Hb during TI of 11.8 (9.7, 13.0) g/dL. All patients who achieved TI maintained TI, with a min, max duration of ongoing TI of 15.7+, 39.4+ months (N = 20) (Table 4). The median (min, max) time to last pRBC transfusion prior to TI was 0.9 (0.5, 2.4) months following ZYNTEGLO infusion. For the patients who were evaluable for TI and did not achieve TI (N = 2), a reduction of 32% and 31% in transfusion volume requirements and a reduction of 30% and 26% in transfusion frequency were observed from 6 months post-drug product infusion to last follow-up compared to pre-enrollment requirements.
After ZYNTEGLO infusion, patient iron removal therapy was managed at physician discretion. Thirteen of the 20 patients who achieved TI are not on chelation therapy as of last follow-up. Of these, 9 (9/13 = 69%) patients did not restart chelation. Four patients (4/13 = 31%) restarted and then stopped iron chelation with a median time from last iron chelation use to last follow-up of 22.7 (7.1, 23.4) months. Of the 20 patients who achieved TI, 7 patients (35%) received phlebotomy to remove iron.
Study 2
Study 2 (NCT03207009) is an ongoing Phase 3 open-label, single-arm, 24-month study to evaluate the efficacy of ZYNTEGLO in 18 patients with β-thalassemia requiring regular transfusions and a β0/β0 or non-β0/β0 (IVS-I-110/IVS-I-110 or IVS-I-110/ β0) genotype. Ten out of 18 patients have rolled over into a long-term follow-up study (Study 3, NCT02633943) after Month 24.
The median (min, max) duration of follow-up is 24.6 (4.1, 35.5) months. All patients remain alive at last follow-up. There were no cases of graft-versus-host disease (GVHD), graft failure, or graft rejection in the clinical study.
The efficacy of ZYNTEGLO was established based on achievement of transfusion independence (TI), which is defined as a weighted average Hb ≥ 9 g/dL without any pRBC transfusions for a continuous period of ≥ 12 months at any time during the study, after infusion of ZYNTEGLO. Fourteen patients are evaluable for TI. Of these, 12/14 (86%, 95% CI: 57, 98) achieved TI with a median (min, max) weighted average Hb during TI of 10.20 (9.3, 13.7) g/dL. All patients who achieved TI maintained TI, with a min, max duration of ongoing TI of 12.5+, 32.8+ months (N = 12) (Table 4). The median (min, max) time to last pRBC transfusion prior to TI was 0.8 (0.0, 1.9) months following ZYNTEGLO infusion. For the patients who were evaluable for TI and did not achieve TI (N = 2), a reduction of 92% and 3% in transfusion volume requirements and a reduction of 87% and 21% in transfusion frequency were observed from 6 months post-drug product infusion to last follow-up compared to pre-enrollment requirements.
After ZYNTEGLO infusion, patient iron removal therapy was managed at physician discretion. Seven of the 12 patients who achieved TI are not on chelation therapy as of last follow-up. Of these, three (3/7 = 43%) patients did not restart chelation. Four patients (4/7 = 57%) restarted and then stopped iron chelation with a median time from last iron chelation use to last follow-up of 7.2 (6.0, 21.4) months. Of the 12 patients who achieved TI, one (8%) received phlebotomy to remove iron.
| Study 1* | Study 2* | Overall Results* | |
|---|---|---|---|
| (N = 23) | (N = 18) | (N = 41) | |
| NR = Not reached. Hb = Total Hb. | |||
|
|||
| Transfusion Independence (TI)† | |||
| n/N‡ (%) | 20/22 (91%) | 12/14 (86%) | 32/36 (89%) |
| [95% CI] | [77, 99] | [57, 98] | [74, 97] |
| Weighted Average Total Hb during TI (g/dL) | |||
| n | 20 | 12 | 32 |
| median | 11.8 | 10.2 | 11.5 |
| (min, max) | (9.7, 13.0) | (9.3, 13.7) | (9.3, 13.7) |
| Duration of TI (months)§ | |||
| n | 20 | 12 | 32 |
| median | NR | NR | NR |
| (min, max) | (15.7+, 39.4+) | (12.5+, 32.8+) | (12.5+, 39.4+) |
| HbAT87Q (g/dL) at Month 6 | |||
| n | 18 | 11 | 29 |
| median | 8.9 | 8.9 | 8.9 |
| (min, max) | (5.2, 10.6) | (3.8, 12.0) | (3.8, 12.0) |
| HbAT87Q (g/dL) at Month 24 | |||
| n | 18 | 8 | 26 |
| median | 8.9 | 9.8 | 9.1 |
| (min, max) | (5.0, 11.4) | (7.9, 12.4) | (5.0, 12.4) |
| Hb¶ (g/dL) at Month 6 | |||
| n | 20 | 12 | 32 |
| median | 11.7 | 10.2 | 11.4 |
| (min, max) | (9.3, 13.3) | (8.8, 13.2) | (8.8, 13.3) |
| Hb¶ (g/dL) at Month 24 | |||
| n | 17 | 9 | 27 |
| median | 12.5 | 10.9 | 11.9 |
| (min, max) | (9.5, 13.3) | (9.7, 14.0) | (9.5, 14.0) |
15. References
1 Lai, X., Liu, L., Zhang, Z. et al. Hepatic veno-occlusive disease/sinusoidal obstruction syndrome after hematopoietic stem cell transplantation for thalassemia major: incidence, management, and outcome. Bone Marrow Transplant 56, 1635–1641 (2021).
16. How is Zynteglo supplied
ZYNTEGLO is supplied in up to four infusion bags containing a frozen suspension of genetically modified autologous cells, enriched for CD34+ cells. Each bag contains approximately 20 mL. Each infusion bag is individually packed within an overwrap in a metal cassette. ZYNTEGLO is shipped from the manufacturing facility to the treatment center storage facility in a cryoshipper, which may contain multiple metal cassettes intended for a single patient. A Lot Information Sheet is affixed inside the shipper.
- 20 mL infusion bag, overwrap, and metal cassette (NDC 73554-3111-1)
Match the identity of the patient with the patient identifiers on the metal cassette(s), infusion bag(s), and Lot Information Sheet upon receipt.
- Keep the infusion bag(s) in the metal cassette(s) and store in the vapor phase of liquid nitrogen at less than or equal to -140°C (≤ -220°F) until ready for thaw and administration.
- Thaw ZYNTEGLO prior to infusion [see Dosage and Administration (2.2)].
- Do not re-freeze after thawing.
- Do not irradiate ZYNTEGLO, as this could lead to inactivation.
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Ensure that patients understand the risk of manufacturing failure. In case of manufacturing failure or the need for additional cells, additional cell collection and manufacturing of ZYNTEGLO would be needed [see Dosage and Administration (2.2)].
Prior to treatment, advise patients of the following:
- Risks associated with mobilization and myeloablative conditioning agents [see Dosage and Administration (2.2), Use in Specific Populations (8.1, 8.3)].
- Delayed platelet engraftment – A risk of bleeding exists after myeloablative conditioning and before platelet engraftment and may continue after engraftment in patients who have continued thrombocytopenia [see Warnings and Precautions (5.1)].
- Risk of neutrophil engraftment failure –Patients who experience neutrophil engraftment failure will receive rescue treatment with their back-up collection of CD34+ cells [see Warnings and Precautions (5.2)].
- Risk of insertional oncogenesis – There is a potential risk of insertional oncogenesis after treatment with ZYNTEGLO. Patients should be monitored lifelong. Monitoring will include assessment for hematologic malignancies with a complete blood count at Month 6 and Month 12 and then at least annually for at least 15 years after treatment with ZYNTEGLO. This will include integration site analysis at Months 6, 12, and as warranted [see Warnings and Precautions (5.3)].
Advise patients to seek immediate attention for the following:
- New or worsening bleeding or bruising. Platelet recovery following ZYNTEGLO infusion could be delayed, potentially resulting in an increased risk of bruising or bleeding until platelet recovery has been achieved [see Warnings and Precautions (5.1), Adverse Reactions (6.1)].
Advise patients to:
- Monitor for signs and symptoms of bleeding and have frequent blood draws for platelet counts, until platelet recovery has been achieved [see Warnings and Precautions (5.1)].
- Have their treating physician contact bluebird bio at 1-833-999-6378 if they are diagnosed with a malignancy [see Warnings and Precautions (5.3)].
Advise patients that they should not donate blood, organs, tissues, or cells at any time in the future [see Dosage and Administration (2.3)].
Advise patients that they may test positive for HIV if tested using a PCR assay after being treated with ZYNTEGLO [see Warnings and Precautions (5.6)].
| PATIENT INFORMATION ZYNTEGLO® (pronounced zin-TEH-glo) (betibeglogene autotemcel) |
|---|
| This Patient Information has been approved by the U.S. Food and Drug Administration. Issued: August 2022 |
| What is the most important information I should know about ZYNTEGLO?
ZYNTEGLO may cause the following side effects:
It is important for you to be monitored at least yearly for at least 15 years for any changes to your blood. There is a potential risk of blood cancer associated with this treatment; however, no cases have been seen in studies of ZYNTEGLO. If you are diagnosed with a cancer, have your treating physician contact bluebird bio at 1-833-999-6378. |
| What is ZYNTEGLO?
ZYNTEGLO is a one-time gene therapy to treat beta-thalassemia (also known as beta-thalassemia major or Cooley's Anemia) in patients who require regular transfusions. Beta-thalassemia is caused by a change in the beta-globin gene, which causes the body to produce reduced or no beta-globin. ZYNTEGLO is made specifically for each patient, using the patient's own blood stem cells and adds functional copies of the beta-globin gene to your cells. This may allow you to produce sufficient hemoglobin to stop receiving regular transfusions. |
| How will I get ZYNTEGLO?
Your healthcare providers will give you other medicines, including chemotherapy medicine, as part of your treatment with ZYNTEGLO. It's important to talk to your healthcare provider about the risks and benefits of all medicines involved in your treatment. After receiving the chemotherapy, it may not be possible for you to become pregnant or father a child. You should consider discussing options for fertility preservation with your doctor before treatment. STEP 1: ZYNTEGLO is made specifically for you from your own blood stem cells. Your healthcare provider will collect your blood stem cells though a process called mobilization and apheresis (A-feh-REE-sis). This process takes approximately one week and may need to be repeated. 'Back-up' stem cells (or 'rescue cells') are also collected and stored at the hospital. This is a precaution in case there is a problem in the treatment process. If this happens, your back-up stem cells will be given back to you. If you receive back-up cells, you will have no benefit from ZYNTEGLO. STEP 2: Your blood stem cells will be sent to a manufacturing site where they are used to make ZYNTEGLO. It takes approximately 70-90 days from the time your cells are collected to manufacture and test ZYNTEGLO before it is shipped to your healthcare provider, but the time may vary. STEP 3: Before you receive ZYNTEGLO, your healthcare provider will give you chemotherapy for a few days to make room in the bone marrow. You will be admitted to the hospital for this step and remain in the hospital until after ZYNTEGLO infusion. STEP 4: ZYNTEGLO is given by an intravenous infusion (into your vein). You may receive more than one bag of ZYNTEGLO. Each bag is infused in 30 minutes or less. After ZYNTEGLO infusion, you will stay in the hospital for approximately 3-6 weeks so that your healthcare team can closely monitor your recovery. Your healthcare provider will determine when you can go home. |
What should I avoid after receiving ZYNTEGLO?
|
| What are the possible or reasonably likely side effects of ZYNTEGLO?
The most common side effects of ZYNTEGLO are:
These are not all the possible side effects of ZYNTEGLO. Call your doctor for medical advice about side effects. You may report side effects to the FDA at 1-800-FDA-1088. |
| General information about the safe and effective use of ZYNTEGLO.
It is important that you have regular check-ups with your healthcare provider, including at least annual blood tests, to detect any adverse effects and to confirm that ZYNTEGLO is still working. Talk to your healthcare provider about any concerns. You can ask your healthcare provider for information about ZYNTEGLO that is written for healthcare professionals. For more information, go to ZYNTEGLO.com or call 1-833-666-2583 for bluebird Patient Services (my bluebird support). Manufactured for: bluebird bio, Inc., Somerville, Massachusetts 02145 |
PRINCIPAL DISPLAY PANEL - 20 mL Bag Patient Identifier Label
betibeglogene autotemcel
zynteglo™
Suspension for IV infusion
20 mL containing 2.0 to 20 x 106 cells/mL
(1.7 to 20 x 106 CD34+ cells/mL)
Confirm Patient Identifiers
Last Name: $LastName$
First Name: $First Name$
Date of Birth: $DOB$
bbb Patient ID: $bbb_PatientID$
COI ID: $bbb_COI_ID$
LOT: $LOT$
EXP: $Expiry$
Bag X of X
DIN $DIN1_DIN2$
U.S. Lic. # 2160
bluebirdbio®
Label P/N: XXXXXXX
PRINCIPAL DISPLAY PANEL - 20 mL Bag Label
betibeglogene autotemcel
zynteglo™
Suspension for IV infusion
20 mL containing 2.0 to 20 x 106 cells/mL
(1.7 to 20 x 106 CD34+ cells/mL)
For autologous use only. For intravenous use only. Rx only.
Contains genetically modified autologous hematopoietic stem cells
suspended in cryopreservation solution containing 5% DMSO.
Not evaluated for infectious substances.
Do not irradiate. Do not use an in-line blood filter or infusion pump.
See full prescribing information for dosage and administration.
See Lot Information Sheet for number of infusion bags and CD34+
cells per kg for this patient.
P/N: XXXXXXX
Label P/N: XXXXXXX
Manufactured for: bluebird bio, Inc.
Somerville, MA 02145
PRINCIPAL DISPLAY PANEL - 20 mL Bag Cassette Label
betibeglogene autotemcel
zynteglo™
Suspension for IV infusion
20 mL containing 2.0 to 20 x 106 cells/mL
(1.7 to 20 x 106 CD34+ cells/mL)
For autologous use only. For intravenous use only. Rx only.
Contains genetically modified autologous hematopoietic stem cells
suspended in cryopreservation solution containing 5% DMSO.
Keep infusion bag(s) in the metal cassette(s). Store in the vapor phase of
liquid nitrogen at ≤ -140°C until ready for thaw and administration. Once
thawed do not re-freeze.
See full prescribing information for dosage and administration.
Do not irradiate. Do not use an in-line blood filter or infusion pump.
Not evaluated for infectious substances. No preservatives.
See Lot Information Sheet for number of infusion bags and CD34+ cells
per kg for this patient.
Confirm Patient Identifiers
Last Name: $LastName$
First Name: $First Name$
Date of Birth: $DOB$
bbb Patient ID: $bbb_PatientID$
COI ID: $bbb_COI_ID$
DIN: $DIN1_DIN2$
LOT: $LOT$
EXP: $Expiry$
Bag X of X
U.S.Lic. # 2160
bluebirdbio®
P/N: XXXXXXX
Label P/N: XXXXXXX
Manufactured for: bluebird bio, Inc.
Somerville, MA 02145
1-800-999-6378
ZYNTEGLO.com
| ZYNTEGLO
betibeglogene autotemcel suspension |
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
| Labeler - bluebird bio, Inc. (969116102) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Lonza Houston, Inc | 832903004 | MANUFACTURE(73554-3111) , ANALYSIS(73554-3111) , LABEL(73554-3111) , PACK(73554-3111) , API MANUFACTURE(73554-3111) | |
More about Zynteglo (betibeglogene autotemcel)
- Check interactions
- Compare alternatives
- Side effects
- Dosage information
- During pregnancy
- FDA approval history
- Drug class: miscellaneous uncategorized agents
- En español