Dipentum: Package Insert / Prescribing Info
Package insert / product label
Generic name: olsalazine sodium
Dosage form: capsule
Drug class: 5-aminosalicylates
Medically reviewed by Drugs.com. Last updated on Aug 5, 2024.
On This Page
- Indications and Usage
- Dosage and Administration
- Dosage Forms and Strengths
- Contraindications
- Warnings and Precautions
- Adverse Reactions/Side Effects
- Drug Interactions
- Use In Specific Populations
- Overdosage
- Description
- Clinical Pharmacology
- Nonclinical Toxicology
- Clinical Studies
- How Supplied/Storage and Handling
- Patient Counseling Information
Highlights of Prescribing Information
DIPENTUM (olsalazine sodium) capsules, for oral use
Initial U.S. Approval: 1987
Indications and Usage for Dipentum
DIPENTUM is an aminosalicylate indicated for the maintenance of remission of ulcerative colitis in adult patients who are intolerant of sulfasalazine. (1)
Dipentum Dosage and Administration
Dosage Forms and Strengths
Capsules: 250 mg olsalazine sodium (3)
Contraindications
Warnings and Precautions
- •
- Renal Impairment: Assess renal function at the beginning of treatment and periodically during treatment. Discontinue DIPENTUM if renal function deteriorates while on therapy. (5.1, 7.1)
- •
- Mesalamine-Induced Acute Intolerance Syndrome: Discontinue treatment if acute intolerance syndrome (cramping, acute abdominal pain, bloody diarrhea, sometimes fever, headache and rash) is suspected. (5.2)
- •
- Hypersensitivity Reactions, including myocarditis and pericarditis: Discontinue DIPENTUM if a hypersensitivity reaction is suspected. (5.3)
- •
- Hepatic Failure: Evaluate the risks and benefits of using DIPENTUM in patients with known liver impairment. (5.4)
- •
- Severe Cutaneous Adverse Reactions: Discontinue at the first signs or symptoms of severe cutaneous adverse reactions or other signs of hypersensitivity and consider further evaluation. (5.5)
- •
- Photosensitivity: Avoid sun exposure if pre-existing skin conditions. (5.6)
- •
- Nephrolithiasis: Cases of nephrolithiasis have been reported with the use of mesalamine. Mesalamine-containing stones are undetectable by standard radiography or computed tomography (CT). Ensure adequate hydration during treatment. (5.7)
- •
- Interference with Laboratory Tests: Mesalamine may lead to elevated urinary normetanephrine test results. (5.8)
Adverse Reactions/Side Effects
Most common adverse reactions (≥2%) are: diarrhea, abdominal pain/cramps, nausea, arthralgia/joint pain, rash, upper respiratory infection and depression. (6)
To report SUSPECTED ADVERSE REACTIONS, contact Meda Pharmaceuticals Inc. at 1-888-380-3276 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
- •
- Nephrotoxic Agents including Non-Steroidal Anti-inflammatory Drugs (NSAIDs): Increased risk of nephrotoxicity; monitor for changes in renal function and mesalamine-related adverse reactions. (7.1)
- •
- Azathioprine or 6-Mercaptopurine: Increased risk of blood dyscrasias; monitor complete blood cell counts and platelet counts. (7.2)
- •
- Low Molecular Weight Heparins or Heparinoids: Increased risk of bleeding following neuraxial anesthesia; if possible, discontinue DIPENTUM or closely monitor for bleeding. (7.1)
- •
- Varicella Vaccine: Avoid use for 6 weeks after vaccination. (7.4)
Use In Specific Populations
Geriatric Patients: Increased risk of blood dyscrasias; monitor complete blood cell counts and platelet counts. (8.5)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 7/2024
Full Prescribing Information
1. Indications and Usage for Dipentum
DIPENTUM is indicated for the maintenance of remission of ulcerative colitis in adult patients who are intolerant of sulfasalazine.
2. Dipentum Dosage and Administration
Evaluate renal function before initiating therapy with DIPENTUM [see Warnings and Precautions (5.1)].
The recommended dosage is 500 mg orally twice daily.
Drink an adequate amount of fluids during treatment [see Warnings and Precautions (5.7)].
3. Dosage Forms and Strengths
Capsules: 250 mg olsalazine sodium in beige capsules imprinted with DIPENTUM® 250 mg on the capsule shell
4. Contraindications
DIPENTUM is contraindicated in patients with known or suspected hypersensitivity to salicylates, aminosalicylates, or to any of the excipients in DIPENTUM [see Warnings and Precautions (5.3), Description (11)].
5. Warnings and Precautions
5.1 Renal Impairment
Renal impairment, including minimal change disease, acute and chronic interstitial nephritis, and renal failure have been reported in patients given DIPENTUM or other products that contain mesalamine or are converted to mesalamine. In animal studies, the kidney was the principal organ of mesalamine toxicity [see Nonclinical Toxicology (13.2)].
Evaluate the risks and benefits of using DIPENTUM in patients with known renal impairment or a history of renal disease or taking concomitant nephrotoxic drugs. Evaluate renal function in all patients prior to initiation and periodically while on DIPENTUM therapy. Discontinue DIPENTUM if renal function deteriorates while on therapy [see Drug Interactions (7.1), Use in Specific Populations (8.6)].
5.2 Mesalamine-Induced Acute Intolerance Syndrome
Olsalazine is converted to mesalamine, which has been associated with an acute intolerance syndrome that may be difficult to distinguish from an exacerbation of ulcerative colitis. Symptoms include cramping, acute abdominal pain and bloody diarrhea, sometimes fever, headache, and rash. Monitor patients for worsening of these symptoms while on treatment. If acute intolerance syndrome is suspected, promptly discontinue treatment with DIPENTUM.
5.3 Hypersensitivity Reactions
Some patients who have experienced a hypersensitivity reaction to sulfasalazine may have a similar reaction to DIPENTUM or to other compounds that contain or are converted to mesalamine. Mesalamine‑induced hypersensitivity reactions may present as internal organ involvement, including myocarditis, pericarditis, nephritis, hepatitis, pneumonitis, and hematologic abnormalities. Evaluate patients immediately if signs or symptoms of a hypersensitivity reaction are present. Discontinue DIPENTUM if an alternative etiology for the signs and symptoms cannot be established.
5.4 Hepatic Failure
There have been reports of hepatic failure in patients with pre-existing liver disease who have been administered mesalamine. Because olsalazine is converted to mesalamine, evaluate the risks and benefits of using DIPENTUM in patients with known liver impairment.
5.5 Severe Cutaneous Adverse Reactions
Severe cutaneous adverse reactions, including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), drug reaction with eosinophilia and systemic symptoms (DRESS), and acute generalized exanthematous pustulosis (AGEP) have been reported with the use of mesalamine, the active moiety in DIPENTUM [see Adverse Reactions (6.2)]. Discontinue DIPENTUM at the first signs or symptoms of severe cutaneous adverse reactions or other signs of hypersensitivity and consider further evaluation.
5.6 Photosensitivity
Patients with pre‑existing skin conditions such as atopic dermatitis and atopic eczema have reported more severe photosensitivity reactions. Advise patients to avoid sun exposure, wear protective clothing, and use a broad-spectrum sunscreen when outdoors.
5.7 Nephrolithiasis
Cases of nephrolithiasis have been reported with the use of mesalamine, the active moiety in DIPENTUM, including stones with 100% mesalamine content. Mesalamine‑containing stones are radiotransparent and undetectable by standard radiography or computed tomography (CT). Ensure adequate fluid intake during treatment.
5.8 Interference with Laboratory Tests
Use of DIPENTUM, which is converted to mesalamine, may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection because of the similarity in the chromatograms of normetanephrine and the main metabolite of mesalamine, N‑acetyl‑5‑aminosalicylic acid (N‑Ac‑5‑ASA). Consider an alternative, selective assay for normetanephrine.
6. Adverse Reactions/Side Effects
The following clinically significant adverse reactions are described elsewhere in the labeling:
- •
- Renal impairment [see Warnings and Precautions (5.1)]
- •
- Mesalamine-induced acute intolerance syndrome [see Warnings and Precautions (5.2)]
- •
- Hypersensitivity reactions [see Warnings and Precautions (5.3)]
- •
- Hepatic failure [see Warnings and Precautions (5.4)]
- •
- Severe cutaneous adverse reactions [see Warnings and Precautions (5.5)]
- •
- Photosensitivity [see Warnings and Precautions (5.6)]
- •
- Nephrolithiasis [see Warnings and Precautions (5.7)]
The following adverse reactions have been identified from clinical studies or postmarketing reports of olsalazine. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
In double-blind, placebo- and active-controlled clinical trials of ulcerative colitis, discontinuations due to adverse reactions were reported in 10% of DIPENTUM-treated patients (N=441) and 7% of placebo-treated patients (N=208). Both sulfasalazine-tolerant and intolerant patients were included. The most common adverse reactions leading to discontinuation in DIPENTUM-treated patients were diarrhea/loose stools (6%), abdominal pain (1%), and rash/itching (1%).
In these controlled trials, adverse reactions reported in 1% or more of patients treated with DIPENTUM and greater than placebo are provided in Table 1.
|
||
|
Adverse Reaction |
DIPENTUM |
Placebo |
|
Diarrhea |
11 |
7 |
|
Abdominal pain/cramps |
10 |
7 |
|
Nausea |
5 |
4 |
|
Arthralgia/Joint Pain |
4 |
3 |
|
Rash |
2 |
1 |
|
Upper Respiratory Infection |
2 |
0 |
|
Depression |
2 |
0 |
|
Vomiting |
1 |
0 |
|
Stomatitis |
1 |
0 |
|
Vertigo/Dizziness |
1 |
0 |
|
Itching |
1 |
0 |
Other adverse reactions reported in clinical trials or post-marketing experience:
Blood and Lymphatic System Disorders
aplastic anemia, anemia, eosinophilia, hemolytic anemia, leukopenia, lymphopenia, neutropenia, pancytopenia, reticulocytosis, thrombocytopenia
Cardiac Disorders
chest pains, heart block second degree, myocarditis, palpitations, pericarditis, peripheral edema, shortness of breath, tachycardia
A patient who developed thyroid disease 9 days after starting DIPENTUM was given propranolol and radioactive iodine and subsequently developed shortness of breath and nausea. The patient died 5 days later with signs and symptoms of acute diffuse myocarditis.
Ear and Labyrinth Disorders
tinnitus
Eye Disorders
dry eyes, vision blurred, watery eyes
Gastrointestinal Disorders
abdominal pain (upper), diarrhea with dehydration, dry mouth, epigastric discomfort, flare in symptoms, flatulence, increased blood in stool, pancreatitis, rectal bleeding, rectal discomfort
General Disorders and Administration Site Conditions
fever chills, hot flashes, irritability, pyrexia, rigors
Hepatobiliary Disorders
hepatic enzyme increased, hepatitis (including cholestasis, granulomatous, and non-specific, reactive), increased bilirubin
Reports of hepatotoxicity, including elevated liver function tests (SGOT/AST, SGPT/ALT, GGT, LDH, alkaline phosphatase, bilirubin), jaundice, cholestatic jaundice, cirrhosis, and possible hepatocellular damage including liver necrosis and liver failure. Some of these cases were fatal. One case of Kawasaki-like syndrome, which included hepatic function changes, was also reported.
Immune System Disorders
bronchospasm, erythema nodosum
Musculoskeletal and Connective Tissue Disorders
myalgia, muscle cramps
Nervous System Disorders
insomnia, paraesthesia, peripheral neuropathy, tremors
Psychiatric Disorders
mood swings
Renal and Urinary Disorders
dysuria, hematuria, interstitial nephritis, nephrolithiasis, nephrotic syndrome, proteinuria, urinary frequency
- •
- Urine discoloration occurring ex-vivo caused by contact of mesalamine, including inactive metabolite, with surfaces or water treated with hypochlorite-containing bleach [see Warnings and Precautions (5.7)].
Reproductive System and Breast Disorders
impotence, menorrhagia, reversible oligospermia
Respiratory, Thoracic and Mediastinal Disorders
dyspnea, interstitial lung disease, pleurisy/pleuritis
Skin and Subcutaneous Tissue Disorders
AGEP, alopecia, angioneurotic edema, DRESS, erythema, photosensitivity reaction, SJS/TEN
Vascular Disorders
hypertension, orthostatic hypotension
7. Drug Interactions
7.1 Nephrotoxic Agents, Including Non-Steroidal Anti-Inflammatory Drugs
The concurrent use of mesalamine with known nephrotoxic agents, including non‑steroidal anti‑inflammatory drugs (NSAIDs), may increase the risk of nephrotoxicity. Monitor patients taking nephrotoxic drugs for changes in renal function and mesalamine-related adverse reactions [see Warnings and Precautions (5.1)].
7.2 Azathioprine or 6-Mercaptopurine
The concurrent use of mesalamine with azathioprine or 6‑mercaptopurine and/or any other drugs known to cause myelotoxicity (e.g., thioguanine) may increase the risk for blood disorders, bone marrow failure, and associated complications. If concomitant use of DIPENTUM and azathioprine or 6-mercaptopurine cannot be avoided, monitor blood tests, including complete blood cell counts and platelet counts.
7.3 Low Molecular Weight Heparins or Heparinoids
The co-administration of salicylates and low molecular weight heparins or heparinoids may result in an increased risk of bleeding (i.e., hematomas) following neuraxial anesthesia. Discontinue DIPENTUM prior to the initiation of a low molecular weight heparin or heparinoid. If this is not possible, it is recommended to monitor patients closely for bleeding.
7.4 Varicella Vaccine
Avoid DIPENTUM, and other salicylates, for six weeks after the varicella vaccine to avoid a possible increased risk of developing Reye’s syndrome.
7.5 Interference With Urinary Normetanephrine Measurements
Use of DIPENTUM, which is converted to mesalamine, may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection [see Warnings and Precautions (5.8)]. Consider an alternative, selective assay for normetanephrine.
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
Published data from meta-analyses, cohort studies and case series on the use of mesalamine, the active moiety in DIPENTUM, during pregnancy have not reliably informed an association with mesalamine and major birth defects, miscarriage, or adverse maternal or fetal outcomes (see Data). There are adverse effects on maternal and fetal outcomes associated with ulcerative colitis in pregnancy (see Clinical Considerations). In animal reproduction studies, there were adverse developmental effects observed after oral administration of olsalazine sodium in pregnant rats during organogenesis at doses of 5 to 20 times the maximum recommended human dose (see Data).
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-associated maternal and embryo/fetal risk
Published data suggest that increased disease activity is associated with the risk of developing adverse pregnancy outcomes in women with ulcerative colitis. Adverse pregnancy outcomes include preterm delivery (before 37 weeks of gestation), low birth weight (less than 2500 g) infants, and small for gestational age at birth.
Data
Human Data
Published data from meta-analyses, cohort studies and case series on the use of mesalamine, the active moiety in DIPENTUM, during early pregnancy (first trimester) and throughout pregnancy have not reliably informed an association of mesalamine and major birth defects, miscarriage, or adverse maternal or fetal outcomes. There is no clear evidence that mesalamine exposure in early pregnancy is associated with an increased risk in major congenital malformations, including cardiac malformations. Published epidemiologic studies have important methodological limitations which hinder interpretation of the data, including inability to control for confounders, such as underlying maternal disease, and maternal use of concomitant medications, and missing information on the dose and duration of use for mesalamine products.
Animal Data
Olsalazine has been shown to produce adverse fetal developmental effects including reduced fetal weights, retarded ossifications, and immaturity of the fetal visceral organs when given during organogenesis to pregnant rats at doses of 100 to 400 mg/kg (5 to 20 times the maximum recommended human dose.
8.2 Lactation
Risk Summary
Data from published literature report the presence of mesalamine and its metabolite, N acetyl-5 aminosalicylic acid, in human milk in small amounts with relative infant doses (RID) of 0.1% or less for mesalamine (see Data). There are case reports of diarrhea in breastfed infants exposed to mesalamine (see Clinical Considerations). There is no information on the effects of the drug on milk production. The lack of clinical data during lactation precludes a clear determination of the risk of DIPENTUM to an infant during lactation; therefore, the developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for DIPENTUM and any potential adverse effects on the breastfed child from DIPENTUM or from the underlying maternal condition.
Data
In published lactation studies, maternal mesalamine doses from various oral and rectal mesalamine formulations and products ranged from 500 mg to 4.8 g daily. The average concentration of mesalamine in milk ranged from non-detectable to 0.5 mg/L. The average concentration of N-acetyl-5-aminosalicylic acid in milk ranged from 0.2 to 9.3 mg/L. Based on these concentrations obtained following administration of oral or rectal mesalamine, the active moiety of olsalazine, estimated infant daily dosages for an exclusively breastfed infant are 0 to 0.075 mg/kg/day (relative infant dose 0 to 0.1% of mesalamine and 0.03 to 1.4 mg/kg/day of N-acetyl-5-aminosalicylic acid).
Oral administration of olsalazine to lactating rats in doses 5 to 20 times the maximum recommended human dose produced growth retardation in the pups.
8.5 Geriatric Use
Clinical studies of DIPENTUM did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Reports from uncontrolled clinical studies and postmarketing reporting systems suggested a higher incidence of blood dyscrasias (i.e., agranulocytosis, neutropenia and pancytopenia) in patients receiving mesalamine-containing products such as DIPENTUM who were 65 years or older compared to younger adult patients, which may also be associated with ulcerative colitis, use of interacting drugs, or reduced renal function.
Consider monitoring of complete blood cell counts and platelet counts in patients 65 years and over during treatment with DIPENTUM. In general, consider the greater frequency of decreased hepatic, renal, or cardiac function, and of concurrent disease or other drug therapy in patients 65 years and over when prescribing DIPENTUM.
8.6 Renal Impairment
Mesalamine is known to be substantially excreted by the kidney, and the risk of adverse reactions to DIPENTUM, which is converted to mesalamine, may be greater in patients with impaired renal function. Evaluate renal function in all patients prior to initiation and periodically while on DIPENTUM therapy. Monitor patients with known renal impairment or history of renal disease or taking nephrotoxic drugs for decreased renal function and mesalamine-related adverse reactions. Discontinue DIPENTUM if renal function deteriorates while on therapy [see Warnings and Precautions (5.1)].
10. Overdosage
DIPENTUM is an aminosalicylate, and symptoms of salicylate toxicity include: nausea, vomiting and abdominal pain, tachypnea, hyperpnea, tinnitus, and neurologic symptoms (headache, dizziness, confusion, seizures). Severe salicylate intoxication may lead to electrolyte and blood pH imbalance and potentially to other organ (e.g., renal and liver) damage.
There is no specific antidote for olsalazine overdose; however, conventional therapy for salicylate toxicity may be beneficial in the event of acute overdosage and may include gastrointestinal tract decontamination to prevent of further absorption. Correct fluid and electrolyte imbalance by the administration of appropriate intravenous therapy and maintain adequate renal function.
11. Dipentum Description
The active ingredient in DIPENTUM (olsalazine sodium) is the sodium salt of a salicylate, disodium 3,3'-azobis (6-hydroxybenzoate) a compound that is effectively bioconverted to mesalamine (5-aminosalicylic acid,5-ASA), an aminosalicylate. Its empirical formula is C14H8N2Na2O6 with a molecular weight of 346.21.
The structural formula is:
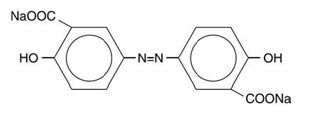
Olsalazine sodium is a yellow crystalline powder, which melts with decomposition at 240°C. It is the sodium salt of a weak acid, soluble in water and DMSO, and practically insoluble in ethanol, chloroform, and ether. Olsalazine sodium has acceptable stability under acidic or basic conditions.
DIPENTUM is supplied in capsules for oral administration. Each DIPENTUM hard gelatin capsule contains 250 mg olsalazine sodium (equivalent to 233.4 mg of olsalazine). The inert ingredient in each capsule is magnesium stearate. The capsule shell contains the following inactive ingredients: black iron oxide, caramel, gelatin, and titanium dioxide.
12. Dipentum - Clinical Pharmacology
12.1 Mechanism of Action
Upon reaching the colon, colonic bacteria convert olsalazine into 5‑aminosalicylic acid (5-ASA or mesalazine). The mechanism of action of 5-ASA (mesalamine) is not fully understood, but appears to be a topical anti-inflammatory effect on colonic epithelial cells. Mucosal production of arachidonic acid metabolites, both through the cyclooxygenase pathways (i.e., prostanoids) and through the lipoxygenase pathways (i.e., leukotrienes and hydroxyeicosatetraenoic acids) is increased in patients with ulcerative colitis, and it is possible that mesalamine diminishes inflammation by blocking cyclooxygenase and inhibiting prostaglandin production in the colon.
12.2 Pharmacodynamics
The exposure-response relationship and time course of pharmacodynamic response for the safety and effectiveness of mesalamine have not been fully characterized.
12.3 Pharmacokinetics
Olsalazine
The usual dose of sulfasalazine for maintenance of remission in patients with ulcerative colitis is 2 grams daily, which would provide approximately 0.8 gram of mesalamine to the colon. More than 0.9 gram of mesalamine would usually be made available in the colon from 1 gram of olsalazine. Patients on daily doses of 1 g olsalazine for 2 to 4 years show a stable plasma concentration of olsalazine-S (3.3 to 12.4 micromol/L).
Absorption
Based on oral and intravenous dosing studies, approximately 2.4% of a single 1 g oral dose is absorbed. Following oral administration of olsalazine, the 98 to 99% of a dose will reach the colon, where each molecule is rapidly converted into two molecules of 5‑ aminosalicylic acid (5-ASA) by colonic bacteria and the low prevailing redox potential found in this environment. The liberated 5-ASA is absorbed slowly resulting in very high local concentrations in the colon. The pharmacokinetics of olsalazine are similar in both healthy volunteers and in patients with ulcerative colitis. Maximum serum concentrations of olsalazine appear after approximately 1 hour and, even after a 1 g single dose, are low (e.g., 1.6 to 6.2 micromol/L).
Distribution
Olsalazine is more than 99% bound to plasma proteins. It does not interfere with protein binding of warfarin. Olsalazine-O-sulfate (olsalazine-S) is more than 99% bound to plasma proteins. Less than 1% of both olsalazine and olsalazine-S appears undissociated in plasma.
Elimination
Metabolism
The conversion of olsalazine to mesalamine (5-ASA) in the colon is similar to that of sulfasalazine, which is converted into sulfapyridine and mesalamine.
Approximately 0.1% of an oral dose of olsalazine is metabolized in the liver to olsalazine-S.
Excretion
Olsalazine has a very short serum half-life, approximately 0.9 hour. The urinary recovery of olsalazine is below 1%. Total recovery of oral 14C-labeled olsalazine in humans ranges from 90 to 97%.
5-aminosalicylic acid (5-ASA)
Absorption
Serum concentrations of 5-ASA are detected after 4 to 8 hours. The peak levels of 5-ASA after an oral dose of 1 g olsalazine range from 0 to 4.3 micromol/L. No accumulation of 5-ASA or Ac-5-ASA (the major metabolite of 5-ASA) in plasma has been detected.
Elimination
Metabolism
N-acetyl-5-ASA (Ac-5-ASA), the major metabolite of 5-ASA found in plasma and urine, is acetylated (deactivated) in at least two sites, the colonic epithelium and the liver. Ac-5-ASA is found in the serum, with peak values of 1.7 to 8.7 micromol/L after a single 1.0 g dose. Pharmacological activities of Ac-5-ASA are unknown.
Excretion
Approximately 20% of the total 5-ASA is recovered in the urine, where it is found almost exclusively as Ac-5-ASA. Of the total 5-ASA found in the urine, more than 90% is in the form of Ac-5-ASA. Only small amounts of 5-ASA are detected. The remaining 5-ASA is partially acetylated and is excreted in the feces. From fecal dialysis, the concentration of 5-ASA in the colon following olsalazine has been calculated to be 18 to 49 micromol/L.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In a two year oral carcinogenicity study in rats, olsalazine was administered to male and female Wistar rats at daily doses of 200, 400, and 800 mg/kg/day (approximately 10 to 40 times the maximum human recommended dose, based on a patient weight of 50 kg and a human dose of 1 g). Urinary bladder transitional cell carcinomas were found in three male rats receiving 40 times the human dose and were not found in untreated male controls. In the same study, urinary bladder transitional cell carcinoma and papilloma occurred in 2 untreated control female rats (2%). No such tumors were found in any of the female rats treated at doses up to 40 times the maximum recommended human dose.
In an eighteen-month oral carcinogenicity study in mice, olsalazine was administered to male and female CD-1 mice at daily doses of 500, 1000, and 2000 mg/kg/day (approximately 25 to 100 times the maximum recommended human dose). Liver hemangiosarcomas were found in two male mice (4%) receiving olsalazine at 100 times the maximum recommended human dose, while no such tumor occurred in the other treated male mice groups or any of the treated female mice. The observed incidence of this tumor is within the 4% incidence in historical controls.
13.2 Animal Toxicology and/or Pharmacology
Preclinical subacute and chronic toxicity studies in rats have shown the kidney to be the major target organ of olsalazine toxicity. At an oral daily dose of 400 mg/kg or higher, olsalazine treatment produced nephritis and tubular necrosis in a 4-week study; interstitial nephritis and tubular calcinosis in a 6-month study, and renal fibrosis, mineralization, and transitional cell hyperplasia in a 1-year study.
14. Clinical Studies
Two double-blind controlled trials have demonstrated the efficacy of DIPENTUM as maintenance therapy in patients with ulcerative colitis. In the first trial, patients with ulcerative colitis in remission were randomized to DIPTENUM 500 mg twice daily or placebo, and relapse rates for a six month period of time were compared. For the 52 patients randomized to DIPENTUM, 12 relapses occurred, while for the 49 patients randomized to placebo, 22 relapses occurred. This difference in relapse rates was significant (p<0.02).
In the second trial, 164 patients with ulcerative colitis in remission were randomized to DIPENTUM 500 mg twice daily or sulfasalazine 1 gram twice daily, and relapse rates were compared after six months. The relapse rate for DIPENTUM-treated patients was 19.5% and 12.2% for sulfasalazine-treated patients, a non-significant difference.
16. How is Dipentum supplied
DIPENTUM is supplied as beige colored capsules, containing 250 mg olsalazine sodium imprinted with “DIPENTUM® 250 mg” on the capsule shell, available as:
Bottles of 100’s NDC 0037-6860-10
Store at 20°C to 25°C (68°F to 77°F). Excursions permitted to 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature].
17. Patient Counseling Information
Renal Impairment
Inform patients that DIPENTUM may decrease their renal function, especially if they have known renal impairment or are taking nephrotoxic drugs, and periodic monitoring of renal function will be performed while they are on therapy. Advise patients to complete all blood tests ordered by their healthcare provider [see Warnings and Precautions (5.1)].
Mesalamine-Induced Acute Intolerance Syndrome and Other Hypersensitivity Reactions
Instruct patients to stop taking DIPENTUM and report to their healthcare provider if they experience new or worsening symptoms of acute intolerance syndrome (cramping, abdominal pain, bloody diarrhea, fever, headache, and rash) or other symptoms suggestive of mesalamine-induced hypersensitivity [see Warnings and Precautions (5.2, 5.3)].
Hepatic Failure
Advise patients with known liver disease to contact their healthcare provider if they experience signs or symptoms of worsening liver function [see Warnings and Precautions (5.4)].
Severe Cutaneous Adverse Reactions
Inform patients of the signs and symptoms of severe cutaneous adverse reactions. Instruct patients to stop taking DIPENTUM and report to their healthcare provider at first appearance of a severe cutaneous adverse reaction or other sign of hypersensitivity [see Warnings and Precautions (5.5)].
Photosensitivity
Advise patients with pre-existing skin conditions to avoid sun exposure, wear protective clothing, and use a broad-spectrum sunscreen when outdoors [see Warnings and Precautions (5.6)].
Nephrolithiasis
Instruct patients to drink an adequate amount of fluids during treatment in order to minimize the risk of kidney stone formation and to contact their healthcare provider if they experience signs or symptoms of a kidney stone (e.g., severe side or back pain, blood in the urine) [see Warnings and Precautions (5.7)].
Blood Disorders
Inform elderly patients and those taking azathioprine or 6-mercaptopurine of the risk for blood disorders and the need for periodic monitoring of complete blood cell counts and platelet counts while on therapy. Advise patients to complete all blood tests ordered by their healthcare provider [see Drug Interactions (7.2), Use in Specific Populations (8.5)].
Administration
- •
- Instruct patients to drink an adequate amount of fluids during treatment.
- •
- Advise patients that urine may become discolored reddish-brown while taking DIPENTUM when it comes in contact with surfaces or water treated with hypochlorite-containing bleach. If discolored urine is observed, advise patients to observe their urine flow. Report to the healthcare provider only if urine is discolored on leaving the body, before contact with any surface or water (e.g., in the toilet) [see Dosage and Administration (2)].
Manufactured for:
MEDA
PHARMACEUTICALS
Canonsburg, PA 15317 U.S.A.
Manufactured by:
SOCIETAL™
CDMO
Societal CDMO Gainesville, LLC
Gainesville, GA 30504, USA
© 2024 Viatris Inc.
DIPENTUM is a registered trademark of Alaven Pharmaceutical LLC, a Viatris Company.
Rev. 7/2024
IN-686010-X14
PRINCIPAL DISPLAY PANEL – 250 mg
NDC 0037-6860-10
Dipentum®
(olsalazine sodium)
capsule, gelatin coated
250 mg
Rx only
100 Capsules
USUAL DOSAGE: See package circular
for complete product information.
PHARMACIST: Dispense in a
well-closed container.
Store at 25°C (77°F); excursions
15°-30°C (59°-86°F).
Manufactured for:
MEDA
PHARMACEUTICALS®
Canonsburg, PA 15317 U.S.A.
Manufactured by:
Societal CDMO Gainesville, LLC
Gainesville, GA 30504, USA
©2023 Viatris Inc.
DIPENTUM is a registered trademark
of Alaven Pharmaceutical LLC,
a Viatris Company.
LB-686010-05
6003065-04
| DIPENTUM
olsalazine sodium capsule, gelatin coated |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Labeler - Meda Pharmaceuticals Inc. (051229602) |
More about Dipentum (olsalazine)
- Check interactions
- Compare alternatives
- Pricing & coupons
- Reviews (5)
- Drug images
- Side effects
- Dosage information
- During pregnancy
- Drug class: 5-aminosalicylates
- Breastfeeding
- En español
