ProAmatine: Package Insert / Prescribing Info
Package insert / product label
Generic name: midodrine hydrochloride
Dosage form: tablet
Drug class: Miscellaneous cardiovascular agents
Medically reviewed by Drugs.com. Last updated on Mar 25, 2024.
The ProAmatine brand name has been discontinued in the U.S. If generic versions of this product have been approved by the FDA, there may be generic equivalents available.
On This Page
Warning: Because ProAmatine® can cause marked elevation of supine blood pressure, it should be used in patients whose lives are considerably impaired despite standard clinical care. The indication for use of ProAmatine® in the treatment of symptomatic orthostatic hypotension is based primarily on a change in a surrogate marker of effectiveness, an increase in systolic blood pressure measured one minute after standing, a surrogate marker considered likely to correspond to a clinical benefit. At present, however, clinical benefits of ProAmatine®, principally improved ability to carry out activities of daily living, have not been verified.
ProAmatine Description
Name: ProAmatine®(midodrine hydrochloride) Tablets
Dosage Form: 2.5-mg, 5-mg and 10-mg tablets for oral administration
Active Ingredient: Midodrine hydrochloride, 2.5 mg, 5 mg and 10 mg
Inactive Ingredients: Colloidal Silicone Dioxide NF, Corn Starch NF, FD&C Blue No. 2 Lake (10-mg tablets), FD&C Yellow No. 6 Lake (5-mg tablet), Magnesium Stearate NF, Microcrystalline Cellulose NF, Talc USP
Pharmacological Classification: Vasopressor/Antihypotensive
Chemical Names (USAN: Midodrine Hydrochloride): (1) Acetamide, 2-amino-N-[2-(2,5-dimethoxyphenyl)-2-hydroxyethyl]-monohydrochloride, (±)-;
(2) (±)-2-amino-N-(β-hydroxy-2,5-dimethoxyphenethyl)acetamide monohydrochloride
BAN, INN, JAN: Midodrine
Structural formula:
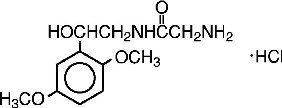
Molecular formula: C12H18N2O4HCl; Molecular Weight: 290.7
Organoleptic Properties: Odorless, white, crystalline powder
Solubility: Water: Soluble
Methanol: Sparingly soluble
pKa: 7.8 (0.3% aqueous solution) pH: 3.5 to 5.5 (5% aqueous solution)
Melting Range: 200 to 203°C
ProAmatine - Clinical Pharmacology
Mechanism of Action: ProAmatine® forms an active metabolite, desglymidodrine, that is an alpha1-agonist, and exerts its actions via activation of the alpha-adrenergic receptors of the arteriolar and venous vasculature, producing an increase in vascular tone and elevation of blood pressure. Desglymidodrine does not stimulate cardiac beta-adrenergic receptors. Desglymidodrine diffuses poorly across the blood-brain barrier, and is therefore not associated with effects on the central nervous system.
Administration of ProAmatine® results in a rise in standing, sitting, and supine systolic and diastolic blood pressure in patients with orthostatic hypotension of various etiologies. Standing systolic blood pressure is elevated by approximately 15 to 30 mmHg at 1 hour after a 10-mg dose of midodrine, with some effect persisting for 2 to 3 hours. ProAmatine® has no clinically significant effect on standing or supine pulse rates in patients with autonomic failure.
Pharmacokinetics:ProAmatine® is a prodrug, i.e., the therapeutic effect of orally administered midodrine is due to the major metabolite desglymidodrine, formed by deglycination of midodrine. After oral administration, ProAmatine® is rapidly absorbed. The plasma levels of the prodrug peak after about half an hour, and decline with a half-life of approximately 25 minutes, while the metabolite reaches peak blood concentrations about 1 to 2 hours after a dose of midodrine and has a half-life of about 3 to 4 hours. The absolute bioavailability of midodrine (measured as desglymidodrine) is 93%. The bioavailability of desglymidodrine is not affected by food. Approximately the same amount of desglymidodrine is formed after intravenous and oral administration of midodrine. Neither midodrine nor desglymidodrine is bound to plasma proteins to any significant extent.
Metabolism and Excretion: Thorough metabolic studies have not been conducted, but it appears that deglycination of midodrine to desglymidodrine takes place in many tissues, and both compounds are metabolized in part by the liver. Neither midodrine nor desglymidodrine is a substrate for monoamine oxidase.
Renal elimination of midodrine is insignificant. The renal clearance of desglymidodrine is of the order of 385 mL/minute, most, about 80%, by active renal secretion. The actual mechanism of active secretion has not been studied, but it is possible that it occurs by the base-secreting pathway responsible for the secretion of several other drugs that are bases (see also Potential for Drug Interactions).
Clinical Studies
Midodrine has been studied in 3 principal controlled trials, one of 3-weeks duration and 2 of 1 to 2 days duration. All studies were randomized, double-blind and parallel-design trials in patients with orthostatic hypotension of any etiology and supine-to-standing fall of systolic blood pressure of at least 15 mmHg accompanied by at least moderate dizziness/lightheadedness. Patients with pre-existing sustained supine hypertension above 180/110 mmHg were routinely excluded. In a 3-week study in 170 patients, most previously untreated with midodrine, the midodrine-treated patients (10 mg t.i.d., with the last dose not later than 6 P.M.) had significantly higher (by about 20 mmHg) 1-minute standing systolic pressure 1 hour after dosing (blood pressures were not measured at other times) for all 3 weeks. After week 1, midodrine-treated patients had small improvements in dizziness/lightheadedness/unsteadiness scores and global evaluations, but these effects were made difficult to interpret by a high early drop-out rate (about 25% vs 5% on placebo). Supine and sitting blood pressure rose 16/8 and 20/10 mmHg, respectively, on average.
In a 2-day study, after open-label midodrine, known midodrine responders received midodrine 10 mg or placebo at 0, 3, and 6 hours. One-minute standing systolic blood pressures were increased 1 hour after each dose by about 15 mmHg and 3 hours after each dose by about 12mmHg; 3-minute standing pressures were increased also at 1, but not 3, hours after dosing. There were increases in standing time seen intermittently 1 hour after dosing, but not at 3 hours.
In a 1-day, dose-response trial, single doses of 0, 2.5, 10, and 20 mg of midodrine were given to 25 patients. The 10- and 20-mg doses produced increases in standing 1- minute systolic pressure of about 30 mmHg at 1 hour; the increase was sustained in part for 2 hours after 10 mg and 4 hours after 20 mg. Supine systolic pressure was =200 mmHg in 22% of patients on 10mg and 45% of patients on 20 mg; elevated pressures often lasted 6 hours or more.
Special Populations
A study with 16 patients undergoing hemodialysis demonstrated that ProAmatine® is removed by dialysis.
Indications and Usage for ProAmatine
ProAmatine® is indicated for the treatment of symptomatic orthostatic hypotension (OH). Because ProAmatine® can cause marked elevation of supine blood pressure (BP>200 mmHg systolic), it should be used in patients whose lives are considerably impaired despite standard clinical care, including non-pharmacologic treatment (such as support stockings), fluid expansion, and lifestyle alterations. The indication is based on ProAmatine®'s effect on increases in 1-minute standing systolic blood pressure, a surrogate marker considered likely to correspond to a clinical benefit. At present, however, clinical benefits of ProAmatine®, principally improved ability to perform life activities, have not been established. Further clinical trials are underway to verify and describe the clinical benefits of ProAmatine®.
After initiation of treatment, ProAmatine® should be continued only for patients who report significant symptomatic improvement.
Contraindications
ProAmatine® is contraindicated in patients with severe organic heart disease, acute renal disease, urinary retention, pheochromocytoma or thyrotoxicosis. ProAmatine® should not be used in patients with persistent and excessive supine hypertension.
Warnings
Supine Hypertension: The most potentially serious adverse reaction associated with ProAmatine® therapy is marked elevation of supine arterial blood pressure (supine hypertension). Systolic pressure of about 200 mmHg were seen overall in about 13.4% of patients given 10 mg of ProAmatine®. Systolic elevations of this degree were most likely to be observed in patients with relatively elevated pre-treatment systolic blood pressures (mean 170 mmHg). There is no experience in patients with initial supine systolic pressure above 180 mmHg, as those patients were excluded from the clinical trials. Use of ProAmatine® in such patients is not recommended. Sitting blood pressures were also elevated by ProAmatine® therapy. It is essential to monitor supine and sitting blood pressures in patients maintained on ProAmatine®.
Precautions
General
The potential for supine and sitting hypertension should be evaluated at the beginning of ProAmatine® therapy. Supine hypertension can often be controlled by preventing the patient from becoming fully supine, i.e., sleeping with the head of the bed elevated. The patient should be cautioned to report symptoms of supine hypertension immediately. Symptoms may include cardiac awareness, pounding in the ears, headache, blurred vision, etc. The patient should be advised to discontinue the medication immediately if supine hypertension persists.
Blood pressure should be monitored carefully when ProAmatine® is used concomitantly with other agents that cause vasoconstriction, such as phenylephrine, ephedrine, dihydroergotamine, phenylpropanolamine, or pseudoephedrine.
A slight slowing of the heart rate may occur after administration of ProAmatine®, primarily due to vagal reflex. Caution should be exercised when ProAmatine® is used concomitantly with cardiac glycosides (such as digitalis), psychopharmacologic agents, beta blockers or other agents that directly or indirectly reduce heart rate. Patients who experience any signs or symptoms suggesting bradycardia (pulse slowing, increased dizziness, syncope, cardiac awareness) should be advised to discontinue ProAmatine® and should be re-evaluated.
ProAmatine® should be used cautiously in patients with urinary retention problems, as desglymidodrine acts on the alpha-adrenergic receptors of the bladder neck.
ProAmatine® should be used with caution in orthostatic hypotensive patients who are also diabetic, as well as those with a history of visual problems who are also taking fludrocortisone acetate, which is known to cause an increase in intraocular pressure and glaucoma.
ProAmatine® use has not been studied in patients with renal impairment. Because desglymidodrine is eliminated via the kidneys, and higher blood levels would be expected in such patients, ProAmatine® should be used with caution in patients with renal impairment, with a starting dose of 2.5 mg (see DOSAGE AND ADMINISTRATION). Renal function should be assessed prior to initial use of ProAmatine®.
ProAmatine® use has not been studied in patients with hepatic impairment. ProAmatine® should be used with caution in patients with hepatic impairment, as the liver has a role in the metabolism of midodrine.
Information for Patients
Patients should be told that certain agents in over-the-counter products, such as cold remedies and diet aids, can elevate blood pressure, and therefore, should be used cautiously with ProAmatine®, as they may enhance or potentiate the pressor effects of ProAmatine® (see Drug Interactions). Patients should also be made aware of the possibility of supine hypertension. They should be told to avoid taking their dose if they are to be supine for any length of time, i.e., they should take their last daily dose of ProAmatine® 3 to 4 hours before bedtime to minimize nighttime supine hypertension.
Laboratory Tests
Since desglymidodrine is eliminated by the kidneys and the liver has a role in its metabolism, evaluation of the patient should include assessment of renal and hepatic function prior to initiating therapy and subsequently, as appropriate.
Drug Interactions
When administered concomitantly with ProAmatine®, cardiac glycosides may enhance or precipitate bradycardia, A.V. block or arrhythmia.
The use of drugs that stimulate alpha-adrenergic receptors (e.g., phenylephrine, pseudoephedrine, ephedrine, phenylpropanolamine or dihydroergotamine) may enhance or potentiate the pressor effects of ProAmatine®. Therefore, caution should be used when ProAmatine® is administered concomitantly with agents that cause vasoconstriction.
ProAmatine® has been used in patients concomitantly treated with salt-retaining steroid therapy (i.e., fludrocortisone acetate), with or without salt supplementation. The potential for supine hypertension should be carefully monitored in these patients and may be minimized by either reducing the dose of fludrocortisone acetate or decreasing the salt intake prior to initiation of treatment with ProAmatine®. Alpha-adrenergic blocking agents, such as prazosin, terazosin, and doxazosin, can antagonize the effects of ProAmatine®.
Potential for Drug Interaction
It appears possible, although there is no supporting experimental evidence, that the high renal clearance of desyglymidodrine (a base) is due to active tubular secretion by the base-secreting system also responsible for the secretion of such drugs as metformin, cimetidine, ranitidine, procainamide, triamterene, flecainide, and quinidine. Thus there may be a potential for drug-drug interactions with these drugs.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies have been conducted in rats and mice at dosages 3 to 4 times the maximum recommended daily human dose on a mg/m2 basis, with no indication of carcinogenic effects related to ProAmatine®. Studies investigating the mutagenic potential of ProAmatine® revealed no evidence of mutagenicity. Other than the dominant lethal assay in male mice, where no impairment of fertility was observed, there have been no studies on the effects of ProAmatine® on fertility.
Pregnancy
Pregnancy Category C. ProAmatine® increased the rate of embryo resorption, reduced fetal body weight in rats and rabbits, and decreased fetal survival in rabbits when given in doses 13 (rat) and 7 (rabbit) times the maximum human dose based on body surface area (mg/m2). There are no adequate and well-controlled studies in pregnant women. ProAmatine® should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. No teratogenic effects have been observed in studies in rats and rabbits.
Adverse Reactions/Side Effects
The most frequent adverse reactions seen in controlled trials were supine and sitting hypertension; paresthesia and pruritus, mainly of the scalp; goosebumps; chills; urinary urge; urinary retention and urinary frequency.
The frequency of these events in a 3-week placebo-controlled trial is shown in the following table:
| Placebo
n=88 | Midodrine
n=82 |
|||
|---|---|---|---|---|
| Event | # of reports | % of patients | # of reports | % of patients |
| Total # of reports | 22 | 77 | ||
| Paresthesia1 | 4 | 4.5 | 15 | 18.3 |
| Piloerection | 0 | 0 | 11 | 13.4 |
| Dysuria2 | 0 | 0 | 11 | 13.4 |
| Pruritis3 | 2 | 2.3 | 10 | 12.2 |
| Supine hypertension4 | 0 | 0 | 6 | 7.3 |
| Chills | 0 | 0 | 4 | 4.9 |
| Pain5 | 0 | 0 | 4 | 4.9 |
| Rash | 1 | 1.1 | 2 | 2.4 |
1 Includes hyperesthesia and scalp paresthesia
2 Includes dysuria (1), increased urinary frequency (2), impaired urination (1), urinary retention (5), urinary urgency (2)
3 Includes scalp pruritus
4 Includes patients who experienced an increase in supine hypertension
5 Includes abdominal pain and pain increase
Less frequent adverse reactions were headache; feeling of pressure/fullness in the head; vasodilation/flushing face; confusion/thinking abnormality; dry mouth; nervousness/anxiety and rash. Other adverse reactions that occurred rarely were visual field defect; dizziness; skin hyperesthesia; insomnia; somnolence; erythema multiforme; canker sore; dry skin; dysuria; impaired urination; asthenia; backache; pyrosis; nausea; gastrointestinal distress; flatulence and leg cramps.
The most potentially serious adverse reaction associated with ProAmatine® therapy is supine hypertension. The feelings of paresthesia, pruritus, piloerection and chills are pilomotor reactions associated with the action of midodrine on the alpha-adrenergic receptors of the hair follicles. Feelings of urinary urgency, retention and frequency are associated with the action of midodrine on the alpha-receptors of the bladder neck.
Overdosage
Symptoms of overdose could include hypertension, piloerection (goosebumps), a sensation of coldness and urinary retention. There are 2 reported cases of overdosage with ProAmatine®, both in young males. One patient ingested ProAmatine® drops, 250 mg, experienced systolic blood pressure greater than 200 mmHg, was treated with an IV injection of 20 mg of phentolamine, and was discharged the same night without any complaints. The other patient ingested 205 mg of ProAmatine® (41 5-mg tablets), and was found lethargic and unable to talk, unresponsive to voice but responsive to painful stimuli, hypertensive and bradycardic. Gastric lavage was performed, and the patient recovered fully by the next day without sequelae.
The single doses that would be associated with symptoms of overdosage or would be potentially life-threatening are unknown. The oral LD50 is approximately 30 to 50 mg/kg in rats, 675 mg/kg in mice, and 125 to 160 mg/kg in dogs.
Desglymidodrine is dialyzable.
Recommended general treatment, based on the pharmacology of the drug, includes induced emesis and administration of alpha-sympatholytic drugs (e.g., phentolamine).
ProAmatine Dosage and Administration
The recommended dose of ProAmatine® is 10 mg, 3 times daily. Dosing should take place during the daytime hours when the patient needs to be upright, pursuing the activities of daily living. A suggested dosing schedule of approximately 4-hour intervals is as follows: shortly before, or upon arising in the morning, midday and late afternoon (not later than 6 P.M.). Doses may be given in 3-hour intervals, if required, to control symptoms, but not more frequently. Single doses as high as 20 mg have been given to patients, but severe and persistent systolic supine hypertension occurs at a high rate (about 45%) at this dose. In order to reduce the potential for supine hypertension during sleep, ProAmatine® should not be given after the evening meal or less than 4 hours before bedtime. Total daily doses greater than 30 mg have been tolerated by some patients, but their safety and usefulness have not been studied systematically or established. Because of the risk of supine hypertension, ProAmatine® should be continued only in patients who appear to attain symptomatic improvement during initial treatment.
The supine and standing blood pressure should be monitored regularly, and the administration of ProAmatine® should be stopped if supine blood pressure increases excessively.
Because desglymidodrine is excreted renally, dosing in patients with abnormal renal function should be cautious; although this has not been systematically studied, it is recommended that treatment of these patients be initiated using 2.5-mg doses.
Dosing in children has not been adequately studied.
Blood levels of midodrine and desglymidodrine were similar when comparing levels in patients 65 or older vs. younger than 65 and when comparing males vs. females, suggesting dose modifications for these groups are not necessary.
How is ProAmatine supplied
ProAmatine® is supplied as 2.5-mg, 5-mg and 10-mg tablets for oral administration. The 2.5-mg tablet is white, round, and biplanar, with a bevelled edge, and is scored on one side with "RPC" above and "2.5" below the score, and "003" on the other side. The 5-mg tablet is orange, round, and biplanar, with a bevelled edge, and is scored on one side with "RPC" above and "5" below the score, and "004" on the other side. The 10-mg is blue, round, and biplanar, with a bevelled edge, and is scored on one side with "RPC" above and "10" below the score, and "007" on the other side.
2.5-milligram Tablets: NDC 54092-003-01 Bottle of 100
5.0-milligram Tablets: NDC 54092-004-01 Bottle of 100
10-milligram Tablets: NDC 54092-007-01 Bottle of 100
Store at 25°C (77°F)
Excursions permitted to 15-30 °C (59-86 °F)
[see USP Controlled Room Temperature]
Manufactured for
Shire US Inc., One Riverfront Place, Newport, KY, 41071, USA
by NYCOMED Austria GmbH
© 2003 Shire US Inc.
Rev. 10/03
003 0107 006
Rx only





| PROAMATINE
midodrine hydrochloride tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| PROAMATINE
midodrine hydrochloride tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| PROAMATINE
midodrine hydrochloride tablet |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Labeler - Shire US Manufacturing Inc. (964907406) |
| Registrant - Shire US Inc. (622467447) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Nycomed Austria GmbH | 300689002 | MANUFACTURE | |
More about ProAmatine (midodrine)
- Check interactions
- Compare alternatives
- Reviews (8)
- Drug images
- Side effects
- Dosage information
- During pregnancy
- Drug class: miscellaneous cardiovascular agents