Artesunate Injection: Package Insert / Prescribing Info
Package insert / product label
Dosage form: injection
Drug class: Miscellaneous antimalarials
Medically reviewed by Drugs.com. Last updated on Oct 31, 2024.
On This Page
- Indications and Usage
- Dosage and Administration
- Dosage Forms and Strengths
- Contraindications
- Warnings and Precautions
- Adverse Reactions/Side Effects
- Drug Interactions
- Use In Specific Populations
- Overdosage
- Description
- Clinical Pharmacology
- Nonclinical Toxicology
- Clinical Studies
- How Supplied/Storage and Handling
- Storage and Handling
- Patient Counseling Information
Highlights of Prescribing Information
ARTESUNATE for injection, for intravenous use
Initial U.S. Approval: 2020
Indications and Usage for Artesunate Injection
Artesunate for Injection is an antimalarial indicated for the initial treatment of severe malaria in adult and pediatric patients. Treatment of severe malaria with Artesunate for Injection should always be followed by a complete treatment course of an appropriate oral antimalarial regimen. (1)
Limitations of Use
Artesunate for Injection does not treat the hypnozoite liver stage forms of Plasmodium and will therefore not prevent relapses of malaria due to Plasmodium vivax or Plasmodium ovale. Concomitant therapy with an antimalarial agent such as an 8-aminoquinoline drug is necessary for the treatment of severe malaria due to P. vivax or P. ovale. (1)
Artesunate Injection Dosage and Administration
- •
- The recommended dosage of Artesunate for Injection is 2.4 mg/kg administered intravenously at 0 hours, 12 hours, and 24 hours, and thereafter administered once daily until the patient is able to tolerate oral antimalarial therapy. (2.1)
- •
- Administer constituted Artesunate for Injection intravenously as a slow bolus over 1 minute to 2 minutes. (2.1)
- •
- Do NOT administer Artesunate for Injection via continuous intravenous infusion. (2.1)
- •
- See the full prescribing information for instructions on preparation and administration of Artesunate for Injection. (2.2)
Dosage Forms and Strengths
For Injection: 110 mg of artesunate as a powder in a single-dose vial for constitution with the supplied sterile diluent. (3)
Contraindications
Serious hypersensitivity to artesunate, such as anaphylaxis. (4)
Warnings and Precautions
- •
- Post-treatment Hemolysis: Cases of post-treatment hemolytic anemia severe enough to require transfusion have been reported. Monitor patients for 4 weeks after treatment for evidence of hemolytic anemia. (5.1)
- •
- Hypersensitivity: Serious hypersensitivity reactions including anaphylaxis have been reported. Discontinue if signs of serious hypersensitivity occur. (5.2)
Adverse Reactions/Side Effects
The most common adverse reactions (incidence of 2% or greater) reported with Artesunate for Injection in clinical trials of severe malaria include acute renal failure requiring dialysis, hemoglobinuria, and jaundice. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Amivas, Inc at [1-855-526-4827 (1-855-5AMIVAS)] or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
Use In Specific Populations
Pregnancy: Based on animal data, may cause fetal harm. However, administration of Artesunate for Injection for the treatment of severe malaria may be lifesaving for the pregnant woman and fetus. Treatment should not be delayed due to pregnancy. (5.3, 8.1)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 10/2021
Full Prescribing Information
1. Indications and Usage for Artesunate Injection
Artesunate for Injection is indicated for the initial treatment of severe malaria in adult and pediatric patients.
Treatment of severe malaria with Artesunate for Injection should always be followed by a complete treatment course of an appropriate oral antimalarial regimen [see Dosage and Administration (2.1)].
Limitations of Use
Artesunate for Injection does not treat the hypnozoite liver stage forms of Plasmodium and will therefore not prevent relapses of malaria due to Plasmodium vivax or Plasmodium ovale. Concomitant therapy with an antimalarial agent such as an 8-aminoquinoline drug is necessary for the treatment of severe malaria due to P. vivax or P. ovale [see Dosage and Administration (2.1)].
2. Artesunate Injection Dosage and Administration
2.1 Recommended Dosage and Administration in Adult and Pediatric Patients
The recommended dosage of Artesunate for Injection is 2.4 mg/kg administered intravenously at 0 hours, 12 hours, and 24 hours, and thereafter, administered once daily until the patient is able to tolerate oral antimalarial therapy.
Administer constituted Artesunate for Injection intravenously as a slow bolus over 1 minute to 2 minutes [see Dosage and Administration (2.2)]. Do NOT administer Artesunate for Injection via continuous intravenous infusion.
Administer Artesunate for Injection with an antimalarial agent that is active against the hypnozoite liver stage forms of Plasmodium, such as an 8-aminoquinoline drug, to patients with severe malaria due to P. vivax or P. ovale.
2.2 Preparation of Artesunate for Injection for Intravenous Administration
Constitution
Artesunate for Injection must be constituted with the supplied diluent prior to administration. A diluent consisting of 12 mL of sterile 0.3 M pH 8.0 sodium phosphate buffer is provided with Artesunate for Injection. To constitute Artesunate for Injection, withdraw 11 mL of this diluent with a needle and syringe and inject into the artesunate vial (when constituted the final concentration of artesunate is 10 mg/mL). Swirl gently (do not shake) for up to 5 to 6 minutes until the powder is fully dissolved and no visible particles remain.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. Do not administer Artesunate for Injection if particulate matter and/or discoloration is observed.
After constitution, inject the constituted solution intravenously (through an established intravenous line or needle) as a slow bolus over 1 to 2 minutes. Discard the vial and any unused portion of the drug product after use.
Storage of the Constituted Solution
Administer the constituted solution within 1.5 hours of constitution with the supplied diluent.
3. Dosage Forms and Strengths
For Injection: 110 mg of artesunate as a sterile white or almost white, fine crystalline powder in a clear glass single-dose vial for constitution.
5. Warnings and Precautions
5.1 Post-Treatment Hemolysis
Post-artesunate delayed hemolysis is characterized by decreased hemoglobin with laboratory evidence of hemolysis (such as decreased haptoglobin and increased lactate dehydrogenase) occurring at least 7 days after initiating artesunate treatment. Cases of post-treatment hemolytic anemia severe enough to require transfusion have been reported [see Adverse Reactions (6.2)]. Monitor patients for 4 weeks after artesunate treatment with Artesunate for Injection for evidence of hemolytic anemia. Since a subset of patients with delayed hemolysis after artesunate therapy have evidence of immune-mediated hemolysis, consider performing a direct antiglobulin test to determine if therapy, e.g. corticosteroids, are necessary.
5.2 Hypersensitivity
Hypersensitivity to artesunate including cases of anaphylaxis have been reported during the use of parenteral artesunate (including Artesunate for Injection) [see Adverse Reactions (6.1, 6.2)]. If hypotension, dyspnea, urticaria, or generalized rash occurs during administration of Artesunate for Injection, consider discontinuing Artesunate for Injection administration and continuing therapy with another antimalarial drug.
5.3 Embryo-Fetal Toxicity in Animals
Extensive experience with oral artesunate and other artemisinin class drugs in pregnant women has not identified a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes.
Animal reproduction studies show that a single intravenous administration of artesunate to rats early in gestation results in embryolethality and oral administration (not an approved route of administration) of artesunate in rats, rabbits, and monkeys induces a dose-dependent increase in embryolethality and fetal malformations. However, the clinical relevance of these data is uncertain [see Use in Specific Populations (8.1)].
Delaying treatment of severe malaria in pregnancy may result in serious morbidity and mortality to the mother and fetus [see Use in Specific Populations (8.1) and Patient Counseling Information (17)].
6. Adverse Reactions/Side Effects
The following clinically significant adverse reactions observed with Artesunate for Injection are discussed in detail in the Warnings and Precautions section:
- •
- Post-treatment Hemolysis [See Warning and Precautions (5.1)]
- •
- Hypersensitivity [See Warning and Precautions (5.2)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described below reflect exposure to intravenous artesunate in a randomized controlled trial in patients with severe malaria in South East Asia, including 730 patients treated with intravenous artesunate (Trial 1), a supportive published randomized, controlled trial of parenteral artesunate in pediatric patients with severe malaria in Africa (Trial 2) and an uncontrolled open label study in the US in 102 patients with severe malaria treated with Artesunate for Injection (Trial 3).
In Trial 1, 730 patients received artesunate 2.4 mg/kg intravenously at 0 hours, 12 hours, 24 hours and then once daily and 730 patients received the comparator quinine as a 20 mg/kg intravenous loading dose then 10 mg/kg intravenously three times daily for treatment of severe malaria in South East Asia. The median age of patients was 28 years (range 2-87 years) and 74% were male, 14% were pediatric patients < 15 years, and 3% were pregnant females. Patients received a median of 3 doses (range 1-9 doses) of intravenous artesunate. Once able to tolerate oral therapy, patients in the artesunate arm received oral artesunate 2 mg/kg daily (not an approved route or dosing regimen) and patients in the quinine arm received oral quinine 10 mg/kg every 8 hours to complete 7 days of total therapy. A subset of patients also received oral doxycycline (100 mg twice daily for 7 days) in addition to oral artesunate or oral quinine.
In Trial 2, pediatric patients younger than 15 years of age with severe malaria in 9 African countries were treated with parenteral artesunate or parenteral quinine.
In Trial 3, 92 of 102 (90%) patients received four 2.4 mg/kg doses of artesunate intravenously at 0 hours, 12 hours, 24 hours, and 48 hours followed by oral antimalarial therapy. The median (range) age of the patients was 39 (1 to 72) years and 61% were male; 63% were African American, 25% were White, and 9% were Asian.
For Trial 1, Trial 2, and Trial 3 adverse reactions were reported during hospitalization and no post-treatment laboratory monitoring was performed.
Most Common Adverse Reactions in Trial 1
The most common adverse reactions (2% or greater) occurring more frequently in patients receiving intravenous artesunate in Trial 1 were dialysis, hemoglobinuria, and jaundice ().
| 1 In Trial 1, 1 patient randomized to the quinine arm did not receive any doses of the study drug. 2 Includes the terms: dialysis, hemodialysis, and peritoneal dialysis. |
||
|
Adverse Reaction |
Artesunate |
Quinine |
|
Acute renal failure requiring dialysis2 |
65 (8.9%) |
53 (7.3%) |
|
Hemoglobinuria |
49 (6.7%) |
33 (4.5%) |
|
Jaundice |
17 (2.3%) |
14 (1.9%) |
Neurologic Sequelae
Patients in Trial 1 were assessed for neurologic sequelae at the time of hospital discharge. The reported neurologic sequelae included loss of balance, hemiplegia/paresis, ataxia, neuropsychiatric symptoms, tremor, generalized weakness, and confusion and restlessness. At hospital discharge, 7 patients (1%) in the artesunate arm had significant neurologic impairments compared with 3 patients (0.4%) in the quinine arm.
Adverse Reactions Reported in Trial 2
In a published randomized controlled open label trial (Trial 2) comparing parenteral artesunate 2.4 mg/kg to parenteral quinine in pediatric patients (<15 years of age) with severe malaria in Africa, the safety profile of intravenous artesunate was generally similar to that described for Trial 1 including greater incidence of neurological impairments at hospital discharge in the artesunate arm compared to the quinine arm.
Most Common Adverse Reactions in Trial 3
The most common adverse reactions in Trial 3 were anemia (65%), transaminase increase (27%), thrombocytopenia (18%), hyperbilirubinemia (14%), acute renal failure (10%), leukocytosis (10%), acute respiratory distress syndrome (8%), lymphopenia (7%), neutropenia (5%), disseminated intravascular coagulation (3%), elevated creatinine (3%), pneumonia (3%), pulmonary edema (3%), and diarrhea (3%).
Clinically Significant Adverse Reactions Reported with Artesunate for Injection in Clinical Trials for Uncomplicated Malaria (not an approved indication) and in Healthy Volunteers
The following clinically significant adverse reactions occurred in ≥ 2% of healthy volunteers or patients:
Blood and lymphatic system disorders: leukopenia, reduced reticulocyte count
Gastrointestinal disorders: abdominal pain, vomiting
General disorders and administration site conditions: pyrexia
Nervous system disorders: dysgeusia, tinnitus, dizziness, and headache
Respiratory, thoracic and mediastinal disorders: cough
Skin and subcutaneous tissue disorders: rash
The following clinically significant reactions occurred in <2% of healthy volunteers or patients:
Immune system disorders: Stevens-Johnson syndrome
Skin and subcutaneous tissue disorders: urticaria
6.2 Postmarketing Experience
The following adverse reactions have been identified during use of parenteral artesunate outside the United States. Because the reactions are reported voluntarily from a population of uncertain size, it is not possible to estimate their frequency reliably or to establish a causal relationship to drug exposure.
Blood and lymphatic system disorders: delayed hemolysis, immune hemolytic anemia
Gastrointestinal disorders: pancreatitis
Immune system disorders: hypersensitivity, anaphylaxis
7. Drug Interactions
7.1 Effect of Other Drugs on Artesunate and Dihydroartemisinin (DHA)
Ritonavir, Nevirapine or Strong UDP-Glucuronosyltransferase (UGT) Inducers:
Published clinical reports or in vitro reports indicate that concomitant use of Artesunate for Injection with oral ritonavir, nevirapine, or UGT inducers may decrease dihydroartemisinin (DHA) AUC and Cmax [see Clinical Pharmacology (12.3)], which may reduce the efficacy of Artesunate for Injection. If Artesunate for Injection is co-administered with ritonavir, nevirapine or strong UGT inducers (e.g., rifampin, carbamazepine, phenytoin), monitor for possible reduced antimalarial efficacy of Artesunate for Injection.
Strong UGT Inhibitors
Published reports of in vitro data indicate that concomitant use of Artesunate for Injection with UGT inhibitors may increase DHA AUC and Cmax [see Clinical Pharmacology (12.3)], which may increase DHA associated adverse reactions. Monitor for adverse reactions when co-administering Artesunate for Injection with strong UGT inhibitors (e.g., axitinib, vandetanib, imatinib, diclofenac).
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
There are serious risks to the mother and fetus associated with untreated severe malaria during pregnancy; delaying treatment of severe malaria in pregnancy may result in serious morbidity and mortality to the mother and fetus (see Clinical Considerations). Pregnancy outcomes reported from a prospective surveillance study with intravenous artesunate are insufficient to identify a drug-associated risk of major birth defects, miscarriage, or fetal death. Experience with oral artesunate (not an approved route of administration) and other artemisinin class drugs (via various routes of administration) in pregnant women over several decades, based on published literature from randomized controlled trials and cohort studies, have not identified a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes (see Data). The bioavailability of oral artesunate is expected to be significantly lower than intravenous artesunate; therefore, the clinical relevance of studies involving oral exposure to artesunate and other artemisinin class drugs is uncertain.
Animal reproduction studies show that a single intravenous administration of artesunate to rats early in gestation results in embryolethality. Oral administration of artesunate during organogenesis in rats, rabbits, and monkeys induces a dose-dependent increase in embryolethality and fetal malformations (e.g., cardiovascular, brain, and/or skeletal) at 0.3- to 1.6-times the clinical dose based on body surface area (BSA) comparisons (see Data). Although animal reproduction studies in several species have demonstrated fetal harm from oral and intravenously administered artesunate and other artemisinin class drugs, the clinical relevance of the animal data is uncertain.
The estimated background risk of miscarriage and maternal and fetal death for the indicated population is higher than the general population. The estimated background risk of major birth defects for the indicated population is unknown. All pregnancies have a background risk of birth defects, loss or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
There is a pregnancy safety study for Artesunate for Injection. If Artesunate for Injection is administered during pregnancy, healthcare providers should report Artesunate for Injection exposure by contacting Amivas, Inc at 1-855-526-4827 (1-855-5AMIVAS) or www.amivas.com/our-products.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk:
Malaria during pregnancy increases the risk for adverse pregnancy outcomes, including maternal anemia, severe malaria, spontaneous abortion, stillbirth, preterm delivery, low birth weight, intrauterine growth restriction, congenital malaria, and maternal and neonatal mortality.
Data
Human Data:
Reports of first trimester use of intravenous artesunate, published randomized control trials, observational studies and cohort studies in over 1300 women exposed to oral artesunate and other artemisinin class drugs (via various routes of administration) in the first trimester of pregnancy and over 6500 women exposed to oral artesunate or other artemisinin class drugs (via various routes of administration) in the second and third trimester of pregnancy have not demonstrated an increase in major birth defects, miscarriage, or adverse maternal or fetal outcomes. The bioavailability of intravenous artesunate is expected to be significantly higher than oral artesunate. Published epidemiologic studies have important methodological limitations which hinder interpretation of data, including inability to control for confounders such as the severity of malaria infection, other underlying maternal diseases, maternal use of concomitant medications, and missing information on the route of administration, dose and duration of use.
Animal Data:
Pregnant rats administered a single dose of intravenous artesunate at 1.5 mg/kg (approximately 0.1 times the clinical dose based on BSA comparisons) early during organogenesis on gestation day (GD) 11 resulted in complete postimplantation loss. A mass balance study conducted in pregnant rats administered a single dose of 5 mg/kg intravenous 14C-artesunate on GD 11 (corresponding to 0.3 times the recommended clinical dose based on BSA comparisons) showed distribution of radiolabeled artesunate (approximately 7% of detected radioactivity) to feto-placental tissues.
Pregnant rats dosed orally during organogenesis (GD 6 through 17) with 6, 10 and 16.7 mg/kg/day artesunate (approximately 0.4- to 1-times the clinical dose based on BSA comparisons) showed dose-dependent post-implantation losses, with surviving fetuses displaying cardiovascular (ventricular septal defects, abnormal origin of subclavian artery) and skeletal (e.g., bent and/or shortened scapulae, humeri, femurs, and fibulae) malformations in the absence of maternal toxicity. Oral dosing in pregnant rabbits during organogenesis (GD 7 through GD 19) at doses of 5, 7, and 12 mg/kg/day artesunate (0.7- to 1.6-times the clinical dose based on BSA comparisons) resulted in cardiovascular (ventricular septal defects, abnormal origin of subclavian artery), skeletal (e.g., cleft sternebrae, shortened and/or displaced ribs) and brain (dilated ventricles, pons absent) malformations in the absence of maternal toxicity. Additionally, administration of artesunate at 12 mg/kg/day to pregnant rabbits during organogenesis resulted in abortions and postimplantation loss. Oral administration of artesunate to pregnant cynomolgus monkeys during organogenesis (GD 20 to GD 50) at 12 mg/kg/day (approximately 1.6-times the clinical dose based on BSA comparisons) resulted in increased embryonic death with skeletal malformations (i.e., decrease in absolute length of the ulna) observed in surviving fetuses.
8.2 Lactation
Risk Summary
DHA, a metabolite of artesunate, is present in human milk. There are no data on the effects of artesunate or DHA on the breastfed infant or on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for Artesunate for Injection and any potential adverse effects on the breastfed child from Artesunate for Injection or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of Artesunate for Injection for the treatment of severe malaria have been established in pediatric patients. Use of Artesunate for Injection for this indication is supported by evidence from adequate and well-controlled studies in adults and pediatric patients with additional pharmacokinetic and safety data in pediatric patients aged 6 months and older [see Adverse Reactions (6.1) and Clinical Studies (14)].
For pediatric patients younger than 6 months of age, a pharmacokinetic (PK) extrapolation approach using modeling and simulation indicated comparable or higher predicted PK steady-state AUC of DHA between this age group and older children or adults at the recommended 2.4 mg/kg dose regimen of Artesunate for Injection. No notable safety issues were identified in limited published safety and outcome data for Artesunate for Injection in pediatric patients younger than 6 months of age with severe malaria. No dose adjustment is necessary for pediatric patients regardless of age or bodyweight [see Dosage and Administration (2.1), Clinical Pharmacology (12.3)].
8.5 Geriatric Use
Clinical studies of Artesunate for Injection did not include sufficient numbers of patients aged 65 years and older to determine whether they respond differently than younger patients.
10. Overdosage
Experience of acute overdose with artesunate is limited. A case of artesunate overdose has been documented in a 5-year-old child inadvertently administered rectal artesunate at a dose of 88 mg/kg/day (approximately 18 times the maximum recommended daily dose for Artesunate for Injection) for 4 days. Artesunate for Injection is not approved for rectal administration. The overdose was associated with pancytopenia, melena, seizures, multiorgan failure and death. Treatment of overdose should consist of general supportive measures.
11. Artesunate Injection Description
Artesunate for Injection 110 mg contains artesunate, a semi-synthetic artemisinin derivative, that is intended for intravenous administration. Artesunate is an antimalarial drug. The structural formula is:
Artesunate is a white or almost white powder with a molecular weight of 384.43. The chemical name is butanedioic acid, mono[(3R,5aS,6R,8aS,9R,10S,12R,12aR)-decahydro-3,6,9-trimethyl-3,12-epoxy-12H-pyrano[4,3-j]-1,2-benzodioxepin-10-yl] ester.
The empirical formula is C19H28O8.
Artesunate for Injection is supplied as white or almost white sterile powder for constitution. Each 20 mL glass single-dose vial contains 110 mg of artesunate for constitution with 11 mL of the supplied sterile diluent. The constituted solution should be a colorless solution.
Each single-dose vial of the supplied sterile diluent contains 12 mL of a sterile diluent. Each 11 mL of the sterile diluent that is used for constitution contains 24.1 mg sodium phosphate monobasic monohydrate and 443.6 mg sodium phosphate dibasic anhydrous in water for injection. Sodium hydroxide and phosphoric acid are used to adjust the pH to 7.9-8.1.
The pH specification for the constituted solution is 7.2-7.7 and the measured osmolality is 305-317 mOsm/kg.
12. Artesunate Injection - Clinical Pharmacology
12.2 Pharmacodynamics
Artesunate and DHA exposure-response relationships and their time course of pharmacodynamic responses are unknown.
Cardiac Electrophysiology
At the approved intravenous dose of 2.4 mg/kg Artesunate for Injection, artesunate and DHA do not cause large mean increases (i.e., 20 msec) in the QTc interval.
12.3 Pharmacokinetics
Following administration of 2.4 mg/kg Artesunate for Injection, artesunate is rapidly converted to DHA by blood esterases. The PK parameters of artesunate (AS) and DHA in patients with severe malaria following administration of multiple doses of 2.4 mg/kg Artesunate for Injection are shown in Table 2.
| PK Parameter | AS | DHA |
|---|---|---|
| PK=pharmacokinetics, AS=artesunate, DHA=dihydroartemisinin, Cmax=maximum concentration, AUC=area under the concentration-time curve | ||
|
Cmax (mcg/mL) |
3.3 (1.0-164) |
3.1 (1.7-9.5) |
|
AUC (mcg-h/mL) |
0.7 (0.3-111.3) |
3.5 (2.2-6.3) |
|
Distribution | ||
|
Volume of Distribution (L) |
68.5 (0.2-818) |
59.7 (26-117) |
|
Protein Binding |
Approximately 93% |
|
|
Elimination | ||
|
Half-life (hours) |
0.3 (0.1-1.8) |
1.3 (0.9-2.9) |
|
Clearance (L/h) |
180 (1-652) |
32.3 (16-55) |
|
In vitro Metabolism | ||
|
Primary Pathway |
Blood Esterases |
Glucuronidation |
|
Metabolite |
DHA |
α-DHA-β-glucuronide |
|
Excretion | ||
|
Urine |
Unknown |
Unknown |
Specific Populations
Pediatric:
PK simulations, using a published population-based meta-analysis of DHA PK indicate a dosing regimen of 2.4 mg/kg results in comparable or greater predicted steady-state DHA AUC0-12 in infants less than 6 month of age compared to that observed in older children or adults (Figure 1). The difference in predicted exposures in infants less than 6 month of age is presumed to be due to immature development of the UGT elimination pathway for DHA.
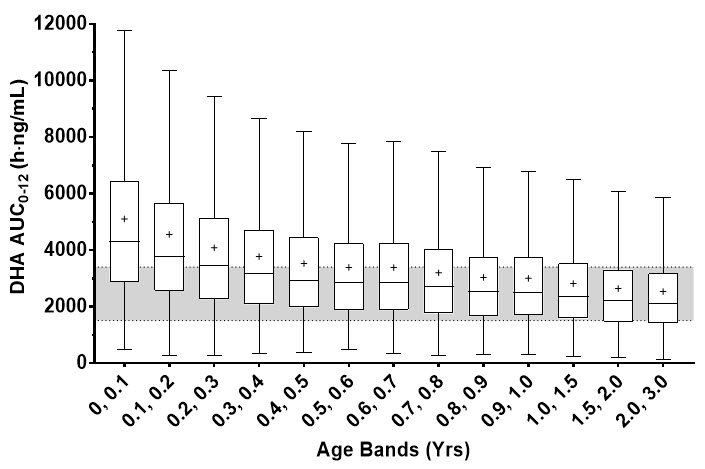
Figure 1. Predicted Steady-State DHA AUC0-12 in Pediatric Patients 0 to 3 Years of Age with Severe Malaria after 2.4 mg/kg Artesunate for Injection
Each box represents the 25th and 75th percentile of the DHA exposure measure. The bar and cross inside the box represent the median and mean respectively, whiskers represent 1.5 times the interquartile range. The gray band represents the interquartile range for patients weighing 20 to 25 kg (8 to 10 years of age) and adults. Clearance was estimated using a combination of allometric weight scaling with a sigmoid function to account for organ maturation.
Pregnant Women:
In a published PK study involving 20 pregnant women with acute uncomplicated malaria administered 4 mg/kg IV artesunate, systemic exposures (Cmax and AUC) of artesunate and DHA were comparable between the pregnant acute malaria patients and the 3-months post-partum healthy patients. Therefore, no dose adjustment is necessary.
Published Clinical Drug-Drug Interaction Studies
Nevirapine:
Co-administration of oral artesunate with nevirapine resulted in a decrease in Cmax and AUC of DHA by 59% and 68%, respectively. This reduction in systemic PK exposure of DHA is also likely to occur with Artesunate for Injection and may result in the potential loss of antimalarial efficacy.
Ritonavir:
Co-administration of oral artesunate with ritonavir resulted in a 27% and 38% decrease in Cmax and AUC, respectively of DHA. This reduction in systemic PK exposure of DHA is also likely to occur with Artesunate for Injection and may result in the potential loss of antimalarial efficacy.
Other Anti-Malarial Drugs:
No clinically significant drug interactions were reported with co-administration of oral artesunate with atovaquone/proguanil, mefloquine, amodiaquine and sulfadoxine/pyrimethamine. Therefore, drug interactions between Artesunate for Injection and these drugs are not expected.
In Vitro Studies:
In vitro studies demonstrated that artesunate and DHA are not metabolized to any significant extent by CYP1A2, 2D6, 2C19, 2A6, 2E1 or 3A; therefore, no dosage adjustments are needed for inhibitors/inducers of these enzymes when co-administered with Artesunate for Injection. DHA is a substrate of UDP-UGT 1A9 or UGT 2B7.
Transporter Systems:
DHA is not a substrate or inhibitor of P-gp or BCRP. Artesunate is a substrate of BCRP and P-gp. Artesunate is a weak inhibitor of OATP1B1 (IC50 = 19 mcg/mL) and OAT3.
12.4 Microbiology
Mechanism of Action
Artesunate is rapidly metabolized into an active metabolite DHA. Artesunate and DHA, like other artemisinins contain an endoperoxide bridge that is activated by heme iron leading to oxidative stress, inhibition of protein and nucleic acid synthesis, ultrastructural changes as well as a decrease in parasite growth and survival.
Both artesunate and DHA are active against the different asexual forms of the Plasmodium parasites and clear parasitemia within 48 to 72 hours.
Antimicrobial Activity
Artesunate and DHA are active against the blood-stage asexual parasites and gametocytes of Plasmodium species including the chloroquine resistant strains [see Clinical Studies (14)]. However, artesunate and DHA are not active against the hypnozoite liver stage forms of P. vivax and P. ovale.
Resistance
There is a potential for development of resistance to artesunate and DHA. Strains of P. falciparum with a decrease in sensitivity to artesunate can be selected in vitro or in vivo. Alterations in some genetic regions of P. falciparum genes such as multidrug resistant 1 (pfmdr1), chloroquine resistance transporter (pfcrt), and kelch13 (K13) have been reported based on in vitro testing and/or identification of isolates in endemic areas where artemisinin therapy has been used.
Recrudescence occurs in patients treated with artesunate monotherapy. Decreased sensitivity to artesunate and other artemisinins, manifesting clinically as slower rates of parasite clearance has been documented in some parts of Southeast Asia and is associated with mutation in the K13 gene.
Cross-resistance
Nonclinical studies in vitro and in malaria animal models suggest a potential for development of cross-resistance with quinine, halofantrine, and amodiaquine. However, the clinical significance of these findings is not known.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies have not been conducted with artesunate.
Mutagenesis
Artesunate was negative in an in vitro bacterial reverse mutation assay, an in vitro Chinese hamster ovary chromosome aberration assay, and an in vivo mouse bone marrow micronucleus assay when administered orally. However, the published literature indicates that artesunate induced DNA damage in human lymphocytes and Hep2G liver cells in a Comet assay and increased micronuclei formation in human lymphocytes. The published literature also indicates that in vivo, artesunate is positive for micronucleus formation but negative for DNA damage in peripheral blood cells in mice following oral administration. No in vivo genetic toxicology studies have been conducted with intravenously administered artesunate.
Fertility
Fertility studies in animals have not been conducted with intravenously administered artesunate.
No significant changes in reproductive organs (i.e., gross, microscopic or histologic lesions or organ weights) or sperm motility, counts or morphology were observed in rats and dogs following 28 days of repeated dosing with intravenously administered artesunate. However, in the published literature, rats and mice administered oral or intraperitoneal artesunate as a single dose or repeated dosing (3 days to 6 weeks) displayed histopathological changes of the seminiferous tubules and altered spermatogenesis (increased percentage of abnormal sperm and/or decreased sperm motility and viability) at doses ranging from approximately 0.2- to 1.3-times the clinical dose based on BSA comparisons. Given the conflicting findings, in the absence of fertility study(ies) conducted with intravenously administered artesunate, the clinical relevance of the animal data on human fertility is uncertain.
14. Clinical Studies
Overview
The efficacy of intravenous artesunate for the treatment of severe malaria was evaluated in a randomized active-controlled trial in Asia (Trial 1) and a supportive published randomized active-controlled trial in Africa (Trial 2).
Trial 1
Trial 1 was an international randomized, open-label, multicenter trial conducted in Bangladesh, India, Indonesia and Myanmar. Hospitalized patients with severe malaria were treated intravenously with either artesunate or quinine. Artesunate was administered at 2.4 mg/kg IV at 0, 12 and 24 hours and then every 24 hours until the patient could tolerate oral medication. Quinine was given IV at 20 mg/kg over 4 hours, followed by 10 mg/kg over 2 to 8 hours, 3 times daily until oral therapy could be started.
Trial 1 consisted of 1461 randomized patients, including 202 pediatric patients <15 years (14%). The median age was 28 years (range 2-87 years) and 74% were male. Malaria was confirmed on blood smear in 1382 patients (95%). Coma was present on admission in 588 patients (40%) and 229 patients (16%) had parasitemia > 10%. Of the 1358 patients with hemoglobin measurement on admission, 94 patients (7%) had documented severe anemia (hemoglobin < 5 g/dL).
Table 3 reports the in-hospital mortality results for Trial 1. The in-hospital mortality rate in the artesunate group (13%) was significantly lower than the rate in the quinine group (21%).
| 1 The odds ratio and 95% CI (confidence interval) were calculated using the Cochran-Mantel-Haenszel approach adjusted by study site. 2 A single patient randomized to quinine arm did not receive any doses of the study drug. |
|||
|
Artesunate |
Quinine |
Odds Ratio (95% CI)1 |
|
|
In-hospital mortality |
96 (13%) |
150 (21%) |
0.59 (0.44, 0.79) |
Trial 2
Additional supportive evidence for efficacy was obtained from a published international, randomized, open-label, multicenter trial comparing parenteral artesunate to parenteral quinine in pediatric patients (< 15 years of age) with severe malaria in nine African countries (Trial 2). Dosing was similar to Trial 1, except that both artesunate and quinine could be administered either intravenously or intramuscularly (not an approved route of administration). Compared to quinine, treatment with artesunate showed a similar advantage with respect to in-hospital mortality as in Trial 1.
16. How is Artesunate Injection supplied
16.1 How Supplied
Artesunate for Injection is supplied as follows:
- •
- 110 mg, white or almost white, sterile, fine crystalline powder for constitution in single-dose, clear glass vials sealed with a rubber stopper (not made with natural rubber latex) and an aluminum overseal
- •
- Clear glass vials of a sterile diluent for constitution are sealed with a rubber stopper (not made with natural rubber latex) and an aluminum overseal.
Artesunate for Injection single-dose vial: NDC 73607-002-01
Sterile Diluent for Constitution single-dose vial: NDC 73607-003-02
Packages of 4 total vials (2 vials of Artesunate for Injection, 110 mg and 2 vials sterile diluent for Artesunate for Injection): NDC 73607-011-11
16.2 Storage and Handling
Store vials of Artesunate for Injection and sterile diluent in the carton at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F) [See USP Controlled Room Temperature]. Do not freeze. Avoid exposure to heat. Keep protected from light. Do not use beyond the expiration date.
17. Patient Counseling Information
Additional Antimalarial Treatment
Advise patients of the need to complete appropriate oral antimalarial therapy after treatment with Artesunate for Injection [see Indications and Usage (1)].
Advise patients of the need to take an additional antimalarial agent such as an 8-aminoquinoline drug during or after treatment with Artesunate for Injection for P. vivax/P. ovale malaria to prevent relapse [see Indications and Usage (1)].
Post-treatment Hemolysis
Advise patients of the need for regular blood tests for the 4-week period following completion of Artesunate for Injection to monitor for post-treatment delayed hemolysis [see Warnings and Precautions (5.1)].
Hypersensitivity Reactions and Anaphylaxis
Inform patients that hypersensitivity reactions, including anaphylaxis, have occurred with administration of Artesunate for Injection. Inform patients of the signs and symptoms of hypersensitivity reactions and anaphylaxis and instruct patients to seek immediate medical care if they experience such symptoms during or following administration of Artesunate for Injection [see Warnings and Precautions (5.2)].
Embryo-Fetal Toxicity in Animals
Advise pregnant patients and patients who could be pregnant of the potential drug-related embryo-fetal toxicity based on animal studies and the serious risks to mother and fetus of delaying treatment for severe malaria. Instruct patients to inform their healthcare provider of a known or suspected pregnancy [see Warnings and Precautions (5.3), Use in Specific Populations (8.1)].
Advise women who are exposed to Artesunate for Injection during pregnancy that there is a pregnancy safety study that monitors pregnancy outcomes. Encourage these patients to report their pregnancy to Amivas, Inc at 1-855-526-4827 (1-855-5AMIVAS) or www.amivas.com/our-products [see Use in Specific Populations (8.1)].
PRINCIPAL DISPLAY PANEL - Carton Label
NDC 73607-011-11 Rx only
Artesunate for Injection
110 mg/vial
Intravenously (slow bolus over 1 minute to 2 minutes)
Each carton contains: 2 vials artesunate, 110 mg and
2 vials sterile diluent for artesunate, 12 mL
Single-dose vial
The vial stopper is not made with natural rubber latex
AMIVAS
| ARTESUNATE
artesunate kit |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Amivas, Inc (116950146) |
More about artesunate
- Check interactions
- Compare alternatives
- Pricing & coupons
- Reviews (1)
- Side effects
- Dosage information
- During pregnancy
- FDA approval history
- Drug class: miscellaneous antimalarials
- Breastfeeding
- En español